



The Pradhan Mantri Matru Vandana Yojana has been in news recently for its meagre financial allocation in Budget 2022-23. Launched in 2017, and now integrated under Mission Shakti, the PMMVY provides Rs 1,000 for early registration of the first pregnancy, Rs 2,000 after an antenatal care check-up six months into pregnancy and Rs 2,000 after childbirth and vaccinations for the newborn.
The aim of the scheme is to improve maternal and child health-related behaviour and to provide partial compensation for income loss so that the mother can take adequate rest before rejoining paid work. Public sector employees and those who receive similar benefits under any other law are excluded.
The controversy erupted when the Narendra Modi government announced that the second pregnancy would also be eligible for cash assistance but only for a girl child. It is not clear how the sex of the second child can be ascertained for the distribution of the first two instalments, given that it is illegal to determine the sex of the unborn baby in India.
Role of community health workers
Notwithstanding these controversies, a crucial aspect of both the PMMVY and the Janani Suraksha Yojana (JSY) — the first-generation maternal conditional cash transfer scheme launched in 2005 that provides Rs 1,000 for delivery in a healthcare institution — remains neglected in the public discourse. This is to do with the crucial role played by the community health workers (CHWs) in making the schemes successful.
The Indian public healthcare system has three main types of CHWs — Auxiliary Nurse Midwife (ANM), Anganwadi workers (AWWs) and the most recent addition of 2005, Accredited Social Health Activists (ASHA). While CHWs provide critical maternal health services to prepare pregnant women for delivery and also provide timely information on a number of maternal and child health-related issues, their contribution is rarely quantified and discussed.
It has been increasingly recognised worldwide that barriers other than the lack of cash, including inadequate information or inaccurate knowledge of health requirements, may undermine investment in children, thereby adversely affecting their health outcomes. Accordingly, to augment the income effects of cash and to induce a behavioural change, both the PMMVY and the JSY have a service component where trained female CHWs act as an interface between mothers and health centres.
These CHWs are also responsible for registering mothers under the programmes, ensuring that they receive antenatal care (ANC) check-ups. Additionally, they also provide advice for institutional delivery, breastfeeding, immunisation and birth control practices among others. The CHWs’ advice, therefore, is likely to complement cash transfer to improve maternal and child health outcomes.
Also read: Electronics, chemicals, machineries set for zero-duty access under India-UAE trade pact
Data on CHWs’ services
To understand the role played by CHWs, we looked at the fourth round of the National Family Health Survey (NFHS-4) of 2015-16 and extracted information on their visits to mothers and their health advice to those who delivered in a public health facility and had a child under the age of 35 months at the time of the survey. This resulted in a sample of 50,076 mother-child pairs in India’s 10 low–performing states (LPS) as defined under the JSY — Uttar Pradesh, Uttarakhand, Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Assam, Rajasthan, Orissa, and Jammu and Kashmir.
The JSY’s focus is on the 10 low-performing states because these had at least three out of four childbirths taking place at home in 2005 when the scheme began. We focus on the financial assistance received for institutional delivery (95 per cent of them were JSY beneficiaries) since data for PMMVY beneficiaries is not collected in the NFHS. However, the beneficiaries are expected to overlap to a large extent, since mothers are encouraged to register for both schemes.
We find that among the mothers who delivered a child in a public healthcare facility and received financial assistance for it, 62 per cent received antenatal care from a CHW during the pregnancy (Table 1). Among those who did not receive financial assistance but delivered in a healthcare facility, 54 per cent received ANC. A majority received ANC from auxiliary nurse midwives followed by Anganwadi workers.
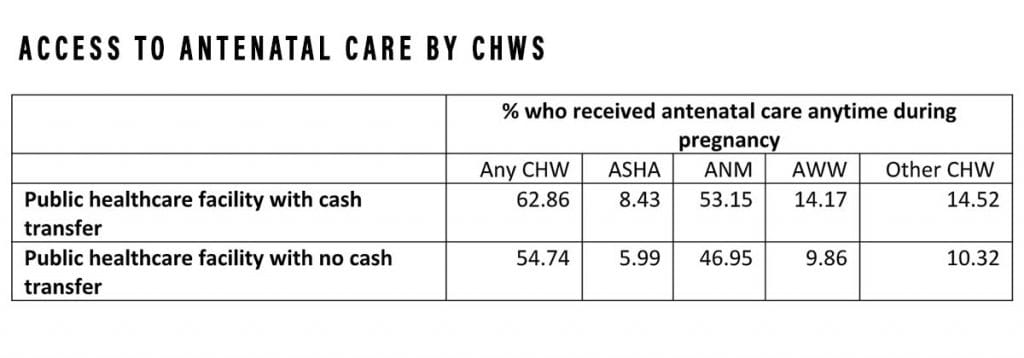
The least proportion of mothers met with an ASHA, the designated CHW under the JSY, even when the delivery was registered under the JSY. About 57 per cent of those receiving financial assistance met with a CHW during the last trimester of pregnancy and around three-fourths received health advice on delivering in a public facility and breastfeeding practices.
Also read: Nursing courses see Covid boom, 99% of BSc seats taken in 2020-21, 91% in diploma
CHW assistance can go a long way
While CHWs’ health advice did not reach nearly half of the mothers who delivered in a public healthcare facility, especially during their last trimester, the complementarity between CHW health advice, cash transfer on health inputs to children such as breastfeeding and immunisation, and health outcomes such as infant mortality rate (IMR) and neonatal mortality rate (NMR) is significant (Table 2).
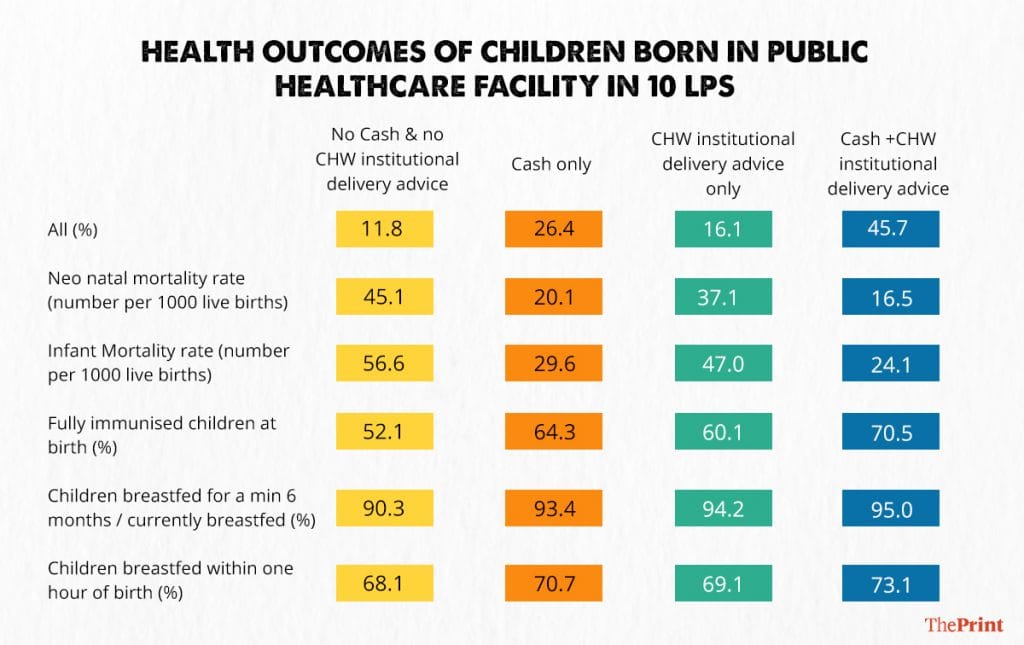
The NMR (number of children who die within 28 days of livebirths) drops from 45 per 1,000 births for children whose mothers neither received cash assistance nor CHW health advice (on institutional delivery) to 16 per 1,000 births for children whose mothers received both.
Similarly, 70 per cent of children whose mothers received both cash assistance and CHW advice, also received all vaccines given at birth — BCG, OPV (polio), Hepatitis B. In contrast, only 50 per cent of children whose mothers did not receive both cash and CHW advice, got all vaccinations given at birth. While the NFHS question specifically asks about the institutional delivery and breastfeeding advice, it is likely that other information such as immunisation, child nutrition, and so on would also be exchanged during a meeting with a CHW.
It is, therefore, important to take into account the complementarity between cash assistance and health advice from CHWs for child health outcomes. India’s public healthcare policies need to expand their reach with an aim of reaching all mothers and strengthening the CHW network to influence early investments in children. CHWs are the unrecognised heroes of the Indian healthcare system.
Sowmya Dhanaraj is Assistant Professor of Economics, Madras School of Economics. Vidya Mahambare is Professor of Economics, Great Lakes Institute of Management. Vibhu Jain is a postgraduate student at Madras School of Economics. Views are personal.
(Edited by Humra Laeeq)