



New Delhi: In 2021, Lakshadweep became India’s first and only union territory (UT) to be declared tuberculosis (TB)-free, four years before India’s target of eliminating tuberculosis by 2025. While India missed that deadline and has since intensified its elimination efforts, Lakshadweep remains the country’s only officially certified TB-free UT.
“Only seven active TB cases have been reported so far in 2026. Last year, 21 cases were reported, all of whom completed treatment and were cured. In 2024, 16 cases were reported,” State TB Officer (STO) for Lakshadweep Dr M.P. Nezeeda told ThePrint Monday.
Lakshadweep’s certification comes under India’s Sub-National Certification system, which recognises districts and UTs that achieve an 80 percent reduction in TB incidence from 2015 levels, a 90 percent reduction in TB deaths, and ensure that no TB-affected household faces catastrophic expenditure because of the disease.
As of mid-2026, no Indian state has achieved TB-free status. However, over 46,118 gram panchayats were awarded TB-free certification for the year 2024, according to a government release.
Now, an upcoming book, Echoes from the Atoll: Inside India’s First TB-Free Islands, due to be launched later this month, revisits how the UT reduced tuberculosis despite it being spread across 10 islands, separated by the Arabian Sea.
Authored by Dr Rakesh P.S., who served as the World Health Organization (WHO) consultant supporting Lakshadweep’s TB programme between 2018 and 2021, the book explains that the achievement did not come through expensive technologies or complex interventions.
Instead, it relied on early diagnosis, repeated door-to-door screening, decentralised testing, integration with primary healthcare and strong community participation.
Tuberculosis is caused by the bacterium mycobacterium tuberculosis and mainly affects the lungs, although it can spread to other organs. It spreads through the air when an infected person with active TB coughs, sneezes or speaks.
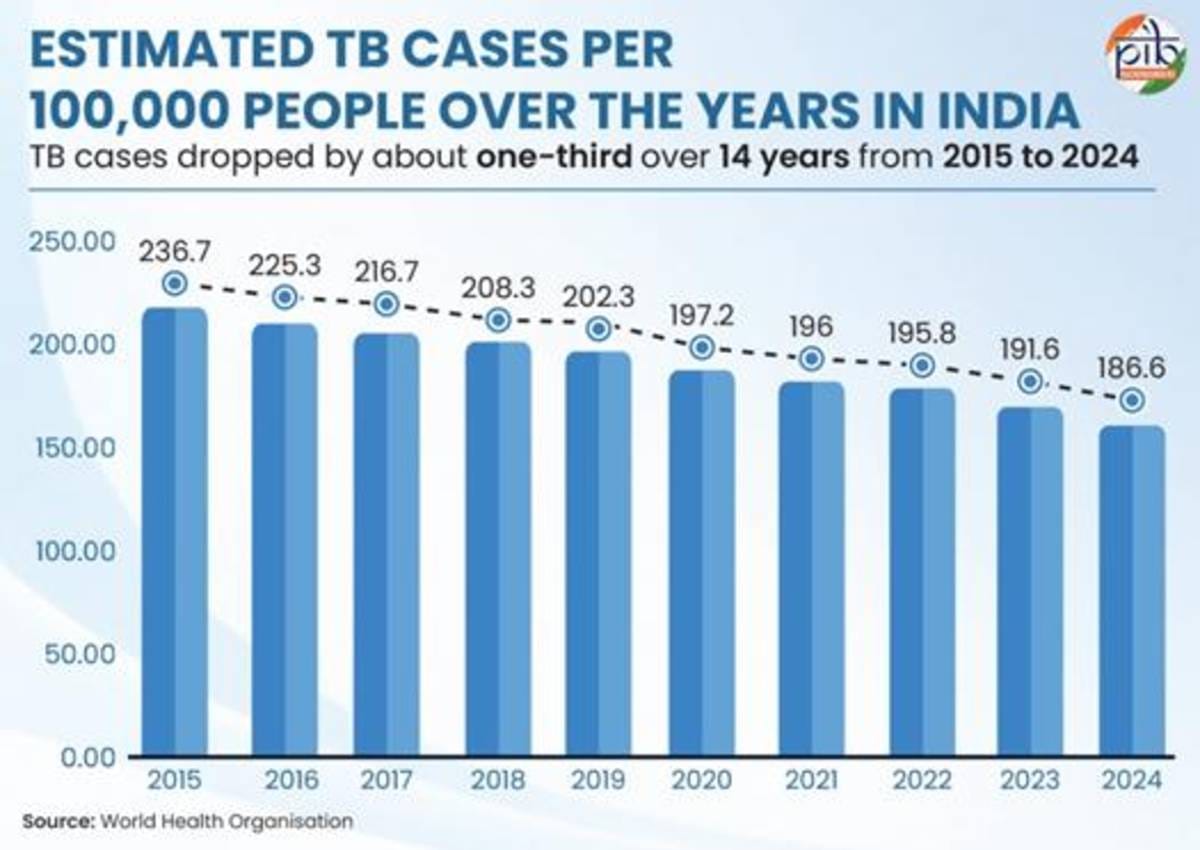
Although India’s TB incidence has dropped by 21% from 237 cases per lakh population in 2015 to 187 cases per lakh population in 2024, according to the ministry of health, the country accounts for roughly a quarter of the global TB burden, making it the highest-burden country worldwide.
WHO defines a “TB-free” region as one reporting fewer than one case per million people each year—a target that no country has achieved.
“The focus should be on reducing TB deaths, preventing financial hardship for families, cutting transmission and ensuring people complete treatment, rather than chasing a numerical definition of elimination,” Dr Rakesh said.
How did Lakshadweep do it?
In Lakshadweep’s TB-elimination programme, geography was the biggest challenge.
The UT has a population of around 70,000 spread across 10 inhabited islands. Dr Rakesh, who later also worked as a global development specialist at the International Union Against Tuberculosis and Lung Diseases, a global scientific organisation, explained that during the monsoon, travel between islands often becomes difficult, delaying movement of patients and laboratory samples.
However, every island already had a primary healthcare facility staffed by doctors, nurses, ASHA workers and multipurpose health workers, many of whom belonged to the local community.
“We customised the strategy based on local realities instead of copying what worked elsewhere,” Dr Rakesh told ThePrint.

Beginning in 2017, health workers carried out repeated rounds of door-to-door screening across all inhabited islands to identify people with TB symptoms. Unlike many states, where active case-finding campaigns focus mainly on selected high-risk groups, Lakshadweep repeatedly screened its entire population.
According to Dr Rakesh, seven consecutive rounds of active case finding helped identify patients early and gradually reduce transmission.
“We don’t need complicated interventions to end TB. We need to find cases early, treat them early and do it consistently over several years,” he said.
The programme was integrated into the primary healthcare system instead of functioning as a separate vertical programme, allowing local health workers to diagnose, monitor and support patients throughout treatment.
Why molecular testing mattered
Another major change was expanding access to molecular tests, which are more accurate than older methods of diagnosing TB.
Traditionally, many TB programmes relied on sputum smear microscopy, where a patient’s sputum (mucus coughed up from the lungs) is examined under a microscope to look for TB bacteria. While this test is inexpensive, it can miss many infections, especially in the early stages of the disease.
Molecular tests such as CBNAAT (Cartridge-Based Nucleic Acid Amplification Test), also known as GeneXpert, and TrueNat, detect the genetic material of the TB bacteria. They are more accurate and can also quickly identify whether the bacteria are resistant to rifampicin, one of the main medicines used to treat TB. This helps doctors start the right treatment sooner.

The WHO explicitly recommends rapid molecular test as the initial diagnostic test for all individuals with signs and symptoms of TB, rather than traditional sputum smear microscopy.
Dr Rakesh said that initially, Lakshadweep had only one GeneXpert machine at its headquarters, making it difficult to transport samples from other islands.
In 2019, however, the programme secured TrueNat machines for individual islands, despite national population norms that would ordinarily have made the UT eligible for only one machine.
According to Dr Rakesh, decentralising molecular testing became one of the programme’s biggest turning points because patients no longer had to wait for samples to travel between islands.
Govt data reflects the shift
In 2020, Lakshadweep still relied largely on smear microscopy, with only 145 of 805 presumptive TB patients—18 percent—tested using molecular methods such as CBNAAT and TrueNat, according to government data.
By 2021, the strategy had changed completely. According to the India TB Report 2022, all 1,045 presumptive TB patients on the islands in 2021 underwent molecular testing, with no microscopy reported.
The approach continued in 2022. The India TB Report 2023 shows all 2,623 presumptive TB patients in 2022 were tested using molecular diagnostics, pushing the screening rate to 3,933 tests per lakh population, among the highest in the country.
This was also the time when Lakshadweep received its TB-free certification.
However, the India TB Report 2024, based on 2023 programme data, shows the testing pattern changed again. Of the 1,048 presumptive TB patients examined, 739 (71 percent) underwent microscopy while 309 (29 percent) received molecular testing. Total screening volume also fell by nearly 60 percent from the previous year.
While Lakshadweep has continued reporting very few TB cases, the reports do not explain the change in pattern.
Official sources said the change in testing pattern in 2023 could be due to a clerical error.
Explaining why Lakshadweep saw a decline in upfront molecular testing in the following years, Dr Nezeeda said that several TrueNat machines had developed recurring technical faults.
“When the machines are not working, we use microscopy initially and send samples to the nearest island where a functioning TrueNat machine is available,” she told ThePrint, adding that ageing machines require frequent repairs and the administration has requested replacements.
Talking about how efforts were sustained even after the TB-free certification, Dr Nezeeda said the UT has continued quarterly active case-finding campaigns, with ASHA workers and other frontline health staff conducting door-to-door screening for TB symptoms in every household.
Also Read: Admitting to slip-ups, Modi govt looks to revise 2025 target for tuberculosis elimination by 2-3 yrs
Community ownership, not just participation
According to Dr Rakesh, another reason for Lakshadweep’s success was that TB control became a community effort rather than remaining solely the responsibility of the health department.

Each island formed a task force comprising local administrators, panchayat representatives, religious leaders, youth groups and health workers. The groups regularly reviewed progress, encouraged people with symptoms to get tested and supported patients through treatment.
“Treatment adherence also became easier because healthcare workers personally knew most residents,” Dr Rakesh said. “The doctors, ASHA workers and nurses knew the patients. The community itself became the treatment support group.
According to Dr Rakesh, Lakshadweep’s high literacy levels and greater participation of women in household health decisions also helped improve treatment completion.
Can the model work elsewhere?
After completing his work in Lakshadweep, Dr Rakesh worked on large-scale TB screening in Delhi’s urban slums, one of the country’s highest-burden settings. There, health workers used AI-enabled handheld X-ray devices that capture a chest X-ray in the field and analyse it instantly using artificial intelligence to identify people who may have TB.
Those flagged by the AI are then referred for confirmatory molecular tests such as TrueNat.

The technology has since become part of India’s post-2025 TB elimination strategy. After missing its target of eliminating TB by 2025, the Centre rolled out a 100-day intensified campaign using around 2,000 AI-enabled handheld X-ray devices to actively screen people in high-risk villages, urban slums, prisons, old-age homes and other vulnerable settings.
Shobha Shukla, chairperson of the Global AMR Media Alliance (GAMA) and lead coordinator of the Prevent-Find-Treat ALL TB campaign, said the shift reflects a broader change in India’s TB programme towards finding cases earlier rather than waiting for patients to seek care.
“On 7 December, 2024, India made a major programmatic shift by deploying AI-enabled X-ray screening among high-risk populations, regardless of whether people had TB symptoms,” she told ThePrint.
She added that India has also rapidly expanded molecular testing and now has around 10,000 WHO-recommended molecular diagnostic machines in the national TB programme, the largest deployment among high-burden countries globally.
“But this is still not enough. In 2024, only 38 percent of people tested for TB across India received an upfront molecular test,” she said, adding that universal access to rapid molecular diagnosis remains critical for early detection.
Drawing on his experience in both Lakshadweep and Delhi, Dr Rakesh said the lesson is not that one model can simply be copied everywhere. “One size does not fit all. Every state has to customise its strategy based on local realities,” he said.
However, he asserted that the core principles remain the same regardless of geography: detect TB early, expand access to molecular testing, start treatment quickly, integrate TB services with primary healthcare and involve communities in supporting patients.
“We don’t need too many interventions. Find TB cases early, treat them early and repeat it consistently. Over time, transmission comes down,” he said.
Shukla said early diagnosis alone is not enough unless patients also receive the right treatment and complete it.
“Every person with TB should receive an early and accurate diagnosis, followed by the right treatment based on drug susceptibility testing so that drug resistance can be prevented,” she said. “Patients also need support to complete the full course of treatment.”
She added that drug-resistant TB is largely preventable and is driven by poor infection control and inappropriate treatment. India also needs to do more to prevent TB by tackling major risk factors such as malnutrition, diabetes, tobacco and alcohol use, and HIV, she underlined.
Even after Lakshadweep was declared TB-free, the UT continued annual active case-finding campaigns. According to Dr Rakesh, the few TB cases now detected are largely among people returning from the mainland or older people with reactivation of latent infection.
“The community should feel it is their responsibility to end tuberculosis. The programme only has to facilitate that ownership,” he said.
(Edited by Nida Fatima Siddiqui)
Also Read: New TB cases in India shot up by 16% in 2018 – but that’s not bad news