



A rare strain of Ebola with no approved vaccine or treatment may have circulated undetected for weeks in conflict-hit northeastern Democratic Republic of Congo before killing at least 80 people.
Laboratory testing by the National Institute for Biomedical Research in Kinshasa confirmed the outbreak is caused by the Bundibugyo strain, the World Health Organization said Friday. The virus has caused only two previous known outbreaks, in Uganda in 2007 and eastern Congo in 2012.
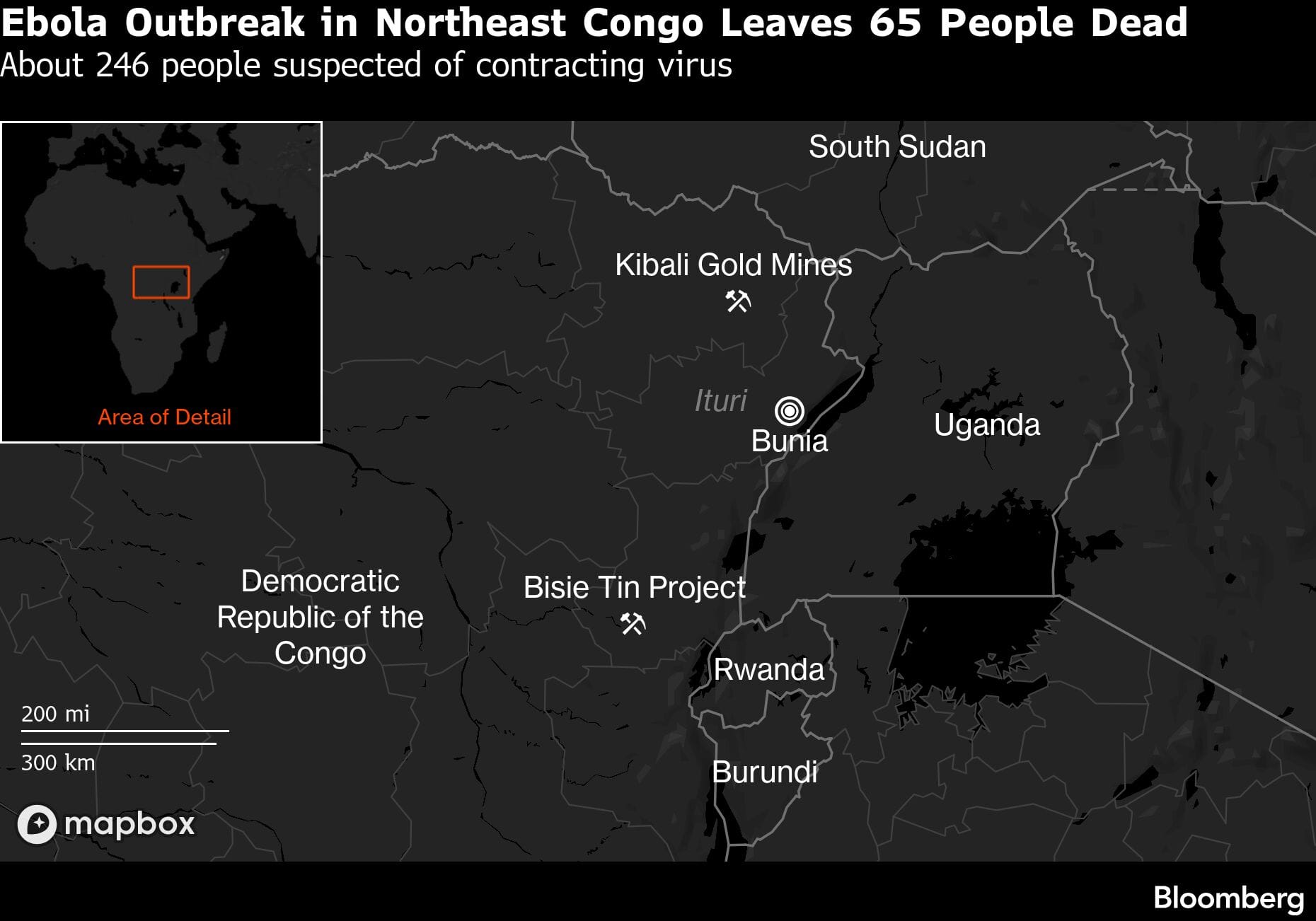
About 246 potential cases have been reported, mainly in Mongbwalu and Rwampara health zones in Ituri province, near the Ugandan border, with additional possible infections in Bunia, the provincial capital, Africa Centres for Disease Control and Prevention said. Four deaths have been confirmed among laboratory-positive cases.
Ebola is among the world’s deadliest infectious diseases, killing between roughly a quarter and almost 90% of infected people depending on the virus species and the medical care available. The Zaire strain, discovered in 1976 near the Ebola River in what is now Democratic Republic of Congo, caused a devastating West African epidemic a decade ago and has received the most research funding, leading to licensed vaccines and treatments.
“Ebola Zaire is the one that got all the attention, for very good reasons,” said Susan McLellan, director of the biocontainment care unit at the University of Texas Medical Branch, in an interview. The development of medical countermeasures, including monoclonal antibodies and vaccines, is less advanced for Bundibugyo, she said.
Clinicians would likely still consider Gilead Sciences Inc.’s remdesivir for Bundibugyo infections, McLellan said. Laboratory research has suggested the strain may be more susceptible to the antiviral than Ebola Zaire.
Uganda Case
Uganda has also confirmed a Bundibugyo Ebola case in a Congolese patient who traveled across the border for treatment and died in intensive care in Kampala on May 14 after deteriorating with bleeding symptoms. Authorities said the body was transported back to Congo the same evening, highlighting the risk of cross-border transmission through movement of patients and infected remains.
WHO is deploying additional epidemiologists, laboratory specialists and infection-control experts to Ituri while airlifting five metric tons of emergency supplies including testing equipment, protective gear and treatment materials, the agency said.
The outbreak is unfolding in a remote part of eastern Congo more than 1,700 kilometers (1,100 miles) from Kinshasa, where insecurity, poor roads, mining-related population movement and frequent cross-border travel complicate the response.
Mongbwalu sits in one of the nation’s gold-mining regions, where tens of thousands of people move between remote mining camps and nearby trading centers. The region is also affected by armed groups and weak infrastructure, complicating efforts to deliver medical supplies and do disease surveillance and contact tracing.
“To access Mongbwalu isn’t easy,” said Jimmy Munguriek, Congo director for advocacy group Resource Matters. “The road isn’t there.”
The area has only one main hospital, Munguriek said, adding that overcrowded mining settlements and constant movement of workers could accelerate transmission if the outbreak isn’t quickly contained.
The US Embassy in Kinshasa warned American citizens Saturday not to travel to Ituri “for any reason,” underscoring concerns over insecurity and limited medical infrastructure in the region.
Escalation Potential
“These zones are full of people who come from everywhere to work in artisanal mining,” Munguriek said. Armed groups active in the area and distrust of health authorities could also hamper containment efforts, he said. “There’s a big risk things will get much worse.”
The scale of the outbreak suggests the virus may have circulated undetected for weeks before being identified. WHO said it first received signals of a suspected outbreak on May 5 and deployed a team to support investigations. Initial tests for the more common Zaire strain were negative, with additional testing later confirming Bundibugyo on May 14.
Congo’s Health Ministry said the presumed first case was a nurse who died at the Evangelical Medical Center in Bunia and dates back to April 24.
“These didn’t all happen in the last week,” McLellan said of the suspected infections. “This has been going on for a while.”
Patients have presented with fever, weakness, vomiting and, in some cases, bleeding, according to WHO, which said several cases rapidly deteriorated and died.
Bodily Fluids
Ebola spreads through direct contact with bodily fluids from infected people or contaminated materials. Transmission risks can rise sharply in settings where people lack reliable access to running water and sanitation, said McLellan, who worked in West Africa during the 2013-2016 Ebola epidemic.
“It takes a very small amount of material,” she said, describing how bodily fluids can remain on skin or surfaces when hand-washing and sanitation are limited.
Even so, experts stressed that Ebola doesn’t spread easily through casual contact and that the risk outside the region remains low.
“There is no documented sustained spread of Ebola outside Africa,” researchers from Imperial College London said in an analysis published Friday, noting that exported cases during the West African epidemic were rare and mostly involved health-care workers.
Congo has extensive experience responding to Ebola outbreaks after battling more than a dozen epidemics over 50 years. The country’s last outbreak, declared over in December, was contained within weeks. Congo’s government said it is deploying rapid-response teams and urged residents to avoid contact with sick people, infected animals and bodily fluids, while thoroughly cooking meat, particularly bush meat.
The outbreak comes as some global health experts warn that cuts to US foreign aid and public health programs could weaken disease surveillance and emergency response capacity in fragile regions. A study published in Science Thursday found the abrupt withdrawal of USAID funding was associated with increased conflict in heavily aid-dependent parts of Africa.
The US Centers for Disease Control and Prevention is “closely monitoring” the outbreak and providing technical support through offices in Congo and Uganda, Acting Director Jay Bhattacharya said Friday.
“We are absolutely involved,” Bhattacharya told reporters Friday. “If we have a safe world, if we can address these needs like the Ebola outbreak, we will also have a safer America.”
–With assistance from Annika Inampudi.
Disclaimer: This report is auto generated from the Bloomberg news service. ThePrint holds no responsibility for its content.