



While the latest coronavirus pandemic rages across the world, India has been no exception to its march. To contain the spread of COVID-19, the Narendra Modi government invoked the 1897 Epidemic Diseases Act which the Britishers had framed to deal with an epidemic that claimed 12 million lives after its initial outbreak in Bombay Presidency in 1896. The historical conditions of its creation as well as the resonances of the Act today warrant a careful study.
In 1896, select British officials were tasked with containing the bubonic plague that first erupted in Bombay Presidency, and soon after raged across the colony. These men observed with alarm a pattern of Gujarati and Marwari grain traders, labourers, Brahmin residents and magistrates fleeing Poona. In his Report on the Outbreak of Bubonic Plague in Bombay, 1897, P.C.H. Snow, the Municipal Commissioner of Bombay, feared, in addition, the rapid flight of cart-drivers, sweepers, cleaners and sanitary workers, for it was this poor, lower caste section of people that the city’s health depended on.
The chairman of the Bombay Plague Committee, Brigadier General W.F. Gatacre, joined Snow in making a fevered case for a strong law that cracked down on people who fled municipal limits. The outcome was the passage of the Epidemic Diseases Act, 1897. The Act has, since then, been invoked to fight dengue and malaria in cities like Chandigarh in 2015, cholera in Vadodara in 2018.

Over 100 years later, on 1 March, 2020, the World Health Organization declared COVID-19 as a pandemic, following which the Modi government announced its decision to invoke the Epidemic Diseases (ED) Act, 1897.
Though the exodus is hardly comparable, there have been many reported instances of people fleeing from quarantine, such as one involving the wife of a Bangalore Google employee, two persons who fled from Jammu, and an American couple from Kerala, all in this month. Section 3 of the Epidemic Diseases Act allows authorities to deem the violation of a regulation to be an offence punishable under Section 188 of the Indian Penal Code. Eventually, the wife and father-in-law of the Google employee was booked under the Epidemic Diseases Act for resisting quarantine and non-cooperation with health officials.
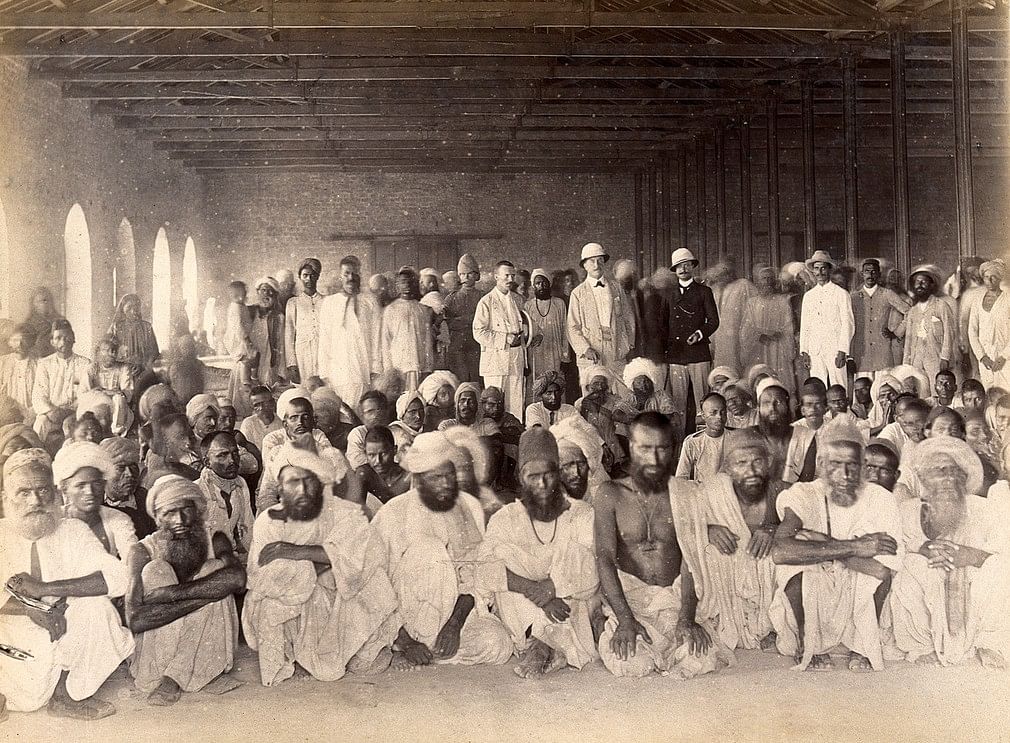
The startling historical conditions that led to the implementation of the Epidemic Diseases Act also saw the creation of an early infrastructure of medical surveillance, involving plague passports, exemption certificates, plague inoculation certificates and above all, detentions.
This infrastructure of medical surveillance was then extended to the presidencies and provinces such as Bengal, Madras, Delhi, Punjab, Central Provinces, and the city of Bangalore in Mysore Residency. Such surveillance was marked by all too common ‘epidemics’ of rumour, official flows of misinformation and a frequent subversion of this infrastructure. Medical surveillance and fake news, quack science, and social panics have resurfaced in similar forms in 2020.
Also read: Karnataka’s Kalaburagi first district to be locked down after India’s first COVID-19 death
How the Epidemic Diseases Act abetted medical surveillance
While the deaths due to COVID-19 have risen globally to 10,405, they nowhere resemble the numbers that the vicious bubonic plague claimed of Indian lives, a staggering 12 million at least across the two decades after 1896.
It is the bubonic plague, caused by the recalcitrant rat flea, and manifesting itself in the form of buboes or swollen lymph nodes, nausea, and fever, that prompted the colonial government of the time to pass the Epidemic Diseases Act. In addition, authorities added ‘bubonic fever’ to the list of infectious or contagious disorders in the Indian Railways Act, 1895.
The combination of both these moves authorised expansive and stringent medical examination and surveillance that included dispatching medical officers for door-to-door examination of bodies, detain and segregate plague suspects at railway stations and ports, and the scrutiny of corpses. In Bombay Presidency, a painstaking system of railways surveillance entailed the creation of certificates of health that attested to the health of all the passengers and railway staff, while Bills of Health signed by the port Health Officers cleared passengers and crew from bubonic plague for travel on steamers. Today, we have the Maharashtra government stamping the left hand of all those who have been sent to home quarantine with indelible ink as a means of curbing the rising trend of fleeing suspects.
In the late 19th century, colonial medical opinion on the extent of stringency to be used varied. The historian, Valeska Huber has argued that colonial medical policy relied to some degree on the strictures of the delegates of the 1897 Venice International Sanitary Conference. These delegates wished the colonial surveillance regime to resemble ‘semi-permeable membranes’ that adopted selective policing rather than be one that was a rigid cordon sanitaire. This meant that colonial authorities were expected to restrict the mobility of certain groups and individuals like the Hajj pilgrim while keeping the borders ‘permeable’ for others.


In the early days after the outbreak, these ideas enjoyed some credence in Bombay Presidency. Third class passengers were examined on the platform, while second class passengers were examined in their carriages, and first class passengers were usually exempted altogether. In Central Provinces, the Chief Commissioner issued orders to not detain all third class passengers, but those ‘regarded by reason of their appearance, by symptoms or dirty conditions of their clothes and effects’. Rather than cancel religious fairs, seen to be glaring sites of potential mass infection, officials often sought to cancel third class railway tickets as they did with the Urs fair held at a dargah in Ajmer in the year 1898.
Medical control was exercised through a bevy of regionally variable identification documents. Madras Presidency introduced plague passports issued to the traveler after she or he had undergone examination and disinfection over 10 days, Bombay Presidency, Bengal Presidency and Punjab issued anti-plague inoculation certificates to those who underwent inoculation. Bombay Presidency issued exemption certificates to those who could provide certificates of health from employers and doctors, permits to regular travelers across causeways after a census, and passes to migrants.
Also read: 1994 Surat plague has many lessons for India on how to beat coronavirus
A bag of assorted tricks
Unsurprisingly, a colorful panoply of petitions, rumour, innuendo, forgery, and a bag of assorted tricks greeted Plague Officers rendering certain practices untenable. If authorities thought they should catch fleeing plague railway suspects, passengers decided that they may as well make the officials run. In response to the practice of plague-marking railway tickets of those who had boarded at infected stations on the Bombay Baroda and Central India (BBCI) Railway Line and the Great Indian Peninsular Railway Line (GIPR), passengers would alight at a station en route and book fresh tickets. And while authorities caught on to this trick and came up with fresh orders to prohibit alighting and booking at intermediate stations, these government regulations caused unspeakable confusion. In some places, such official practices were given up because they were not worth the bother.
The tricks, however, refused to exhaust themselves owing to the large remit of caste, religious taboos and untouchability. The Parsi medical scientist and doctor attached to the Arthur Road Hospital of Bombay during the plague, N.H Choksy wrote that families ended up abandoning, concealing or indiscriminately throwing out their suffering relatives.
These pre-emptive antics were the byproduct of fear of caste pollution, resulting from quarantine in common hospital wards, as well as autopsy and dissection. Procedures such as the insistence on death certificates before corpses could be buried were silently relaxed owing to the simmering anger that the European touching of corpses provoked. Historian David Arnold, in an article titled Touching the Body: Perspectives on the Indian Plague 1896-1900, cites the 6 April 1897 issue of Tilak’s Marathi newspaper Kesari, to narrate the story of a Brahmin who had to live on milk while in hospital because the food had been polluted by a Shudra’s touch. There was outrage against closure of the Hindu Plague hospital, where caste observances were respected, and appreciation for the setting up of caste-based hospitals, 30 of which came up by early 1898.
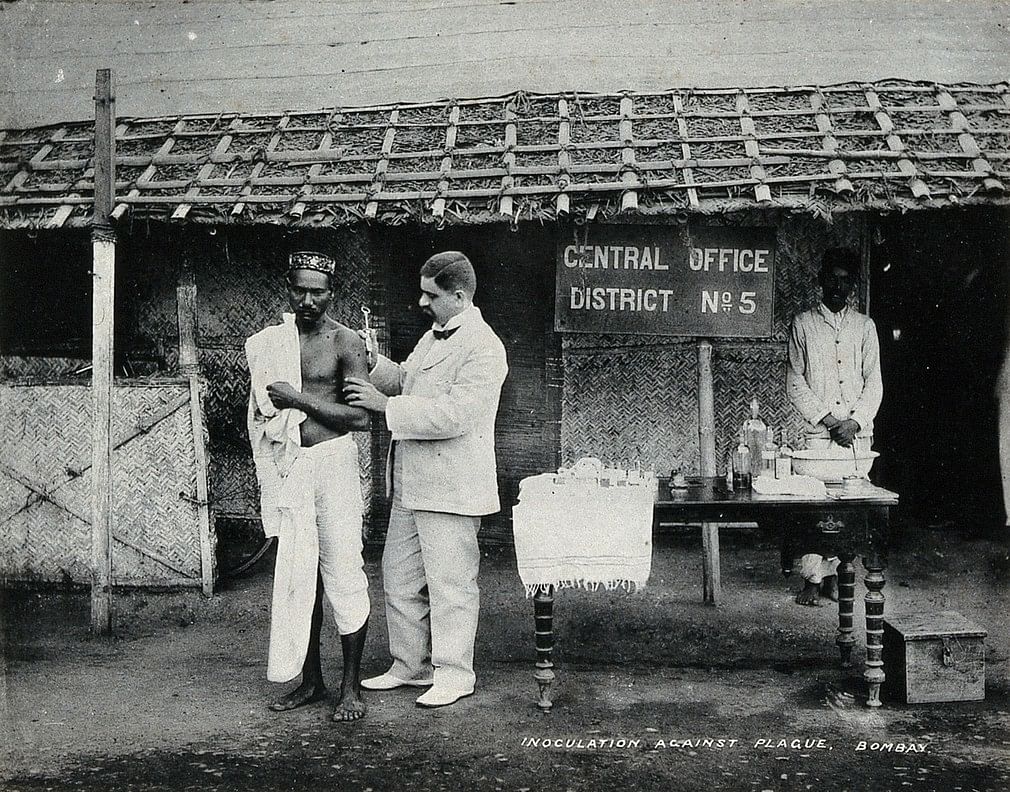
Waves of rumour crashed against just about every medical move of surveillance but particularly those intended at achieving a success rate of inoculation. When the Russian bacteriologist Waldemar Haffkine came up with an inoculation fluid capable of producing resistance to plague, he first tested it on himself and then on the inmates of the Byculla prison in Bombay. But this could not stem the flow of fast-flying rumours that inoculation induced infertility, and so, authorities had to take to calling on a crop of medical practitioners such as vaids and hakims, ‘native gentlemen’ including Tilak and Aga Khan, as volunteers for inoculation.
Printed on the inoculation certificate were several ‘incentives’ such as 4 annas, a day off from work, and exemption from detention for 6 months. W.L. Harvey, the Municipal Commissioner of Bombay in 1900, noted that some Indians underwent inoculation as many as 10-30 times in light of these incentives.
While the colonial establishment complained, these practices must not be seen purely as Indians causing misinformation, but also as providing critical information of socio-cultural prisms such as caste through which Indians act.
Besides, colonial officials were themselves guilty of a chaos of medical doctrines that prevailed, with miasma theory (or the theory that epidemics spread through noxious fumes emerging from cesspools, open drains, slums) firmly ensconcing itself until the arrival of Haffkine’s prophylactic. Bacteriologist Robert Koch, who discovered the cholera bacillus, was greeted with hostility by British administrators like the Sanitary Commissioner J.M. Cuningham, who felt that these findings would engender unnecessary medical quarantines and embargoes on international trade. Limewashing of buildings and eviction of slum residents continued apace even after inoculation was conceived.
Also read: China’s love for wildlife meat to its authoritarianism — how coronavirus got out of hand
Right Wing bio-politics and COVID-19
As we consider the medley of medical surveillance, official medical misinformation and manipulation, it is hard to ignore similar contemporary trends manifest in gaumutra squads, WhatsApp messengers of fake news, and fleeing relatives fearful of government hospitals. Authorities at Delhi’s Nigambodh Ghat refused to carry out the cremation of the only woman to have died in Delhi. Even when an AIIMS doctor, and other high-profile experts asserted that the disease spreads only through ‘respiratory secretion’, which a dead body cannot generate, such fears abound, with state administrations not able to dispel fears.
A scholar of technology and society, Zeynep Tufekci notes, ‘the coronavirus revealed authoritarianism’s fatal flaw’ under Xi Jinping’s rule of containing the disease in China through a regime of surveillance and censorship which refused crucial information shared by whistleblowers and social media. In contrast, the Indian government has enabled misinformation through other means of right-wing bio-politics.
The Akhil Bharat Hindu Mahasabha was recently allowed to host a party where they peddled medical knowledge that drinking gaumutra or cow urine and taking a bath in cow dung would fend off the virus. Meanwhile, fake advisories such as the one touted to be by UNICEF are making the rounds on WhatsApp, urging people to not eat cold foods, frequently wash their clothes, with others calling for the heavy intake of Vitamin C. Popular YouTube channels such as Prajapati News (with 6.21 million subscribers) are showing the virus resulted from a leak in a Chinese government lab experiment intended to attack rival nations.
While the government does little to counter such fake news, it has also encouraged gaumutra theories (through the advocacy of individual BJP party members) as well as the efficacy of homeopathy and other herbal treatments (through the aegis of the AYUSH Ministry). In the face of all this, the imposition of the Epidemic Diseases Act to enforce colonial rule-styled medical surveillance and punishments can only go so far. Hence, investing in a system of public health that improves universal faith in, and access to, government hospitals is essential.
Tarangini Sriraman teaches history and politics at Azim Premji University, Bengaluru. Views are personal.