



A central tenet of democracy is that it enables citizens to reward or punish their lawmakers for delivering, or failing to deliver, essential goods and services that contribute to a society’s health and economic well-being. In principle, lawmakers should be motivated to ensure that frontline workers such as teachers or health workers deliver these goods and services to citizens. However, as we in India know all too well, a large number of factors can get in the way of such accountability. But what if it was possible to implement a better, more direct system of accountability in a manner that is scalable nationally?
A large study that we conducted in rural Uttar Pradesh shows that a system of “social accountability” can lead to significant improvements in key maternal and child health outcomes. Accountability of panchayat leaders and frontline workers was increased by informing citizens about services they were entitled to and by facilitating community meetings that brought them together. Over a period of 1-2 years, our study found that information provision combined with community engagement led to significant improvements in full immunisation rates among young children and higher institutional deliveries among pregnant women.
Social accountability is an innovation in governance that enables members of the local community to hold frontline service providers accountable. One key component of social accountability is providing information to citizens about their community’s health and education outcomes, their rights to receive public sector services, and the responsibilities of panchayat leaders and frontline workers. Another key component is providing citizens with a mechanism for redressal of their grievances, often through facilitated community meetings held on a regular basis. The idea to give power to the people isn’t new – a number of social movements, in India and globally, have been organising public hearings and transparency initiatives.
As part of the World Bank-supported Uttar Pradesh Health Systems Strengthening Project (UPHSSP), we collaborated with UP’s State Institute of Rural Development (SIRD) to help develop a social accountability intervention and rigorously evaluate its impact. The objective of the programme was to improve delivery of key maternal and child health and nutrition services in villages with poor underlying health outcomes and to reduce rates of childhood malnutrition.
Also read: India didn’t create Covid-19 problem, but a better system would’ve helped us cope better
The accountability interventions were designed to be implemented through the village health, sanitation, and nutrition committees (VHSNCs). In 2016, when the interventions were launched, VHSNCs in most of Uttar Pradesh were dormant despite being required as part of the National Health Mission guidelines. These VHSNCs were supposed to be constituted within every gram panchayat, with their members including elected panchayat leaders, ward members, frontline health workers (the ASHA, Aanganwadi worker, and ANM), and community members. The VHSNCs were charged with identifying key health needs in their village(s) and also received Rs 10,000 annually towards discretionary spending. In addition, they also had the authority to alert block-level authorities to health problems and community needs.
At the centre of the intervention was a Gram Panchayat Coordinator (GPC) – a facilitator recruited from the area and trained on the roles and responsibilities of the VHSNC, and frontline health workers. The GPCs were also trained to activate the dormant VHSNC, by visiting each GP, meeting each of the VHSNC members to tell them about their roles and responsibilities on the committee, and facilitating monthly meetings of the VHSNC.
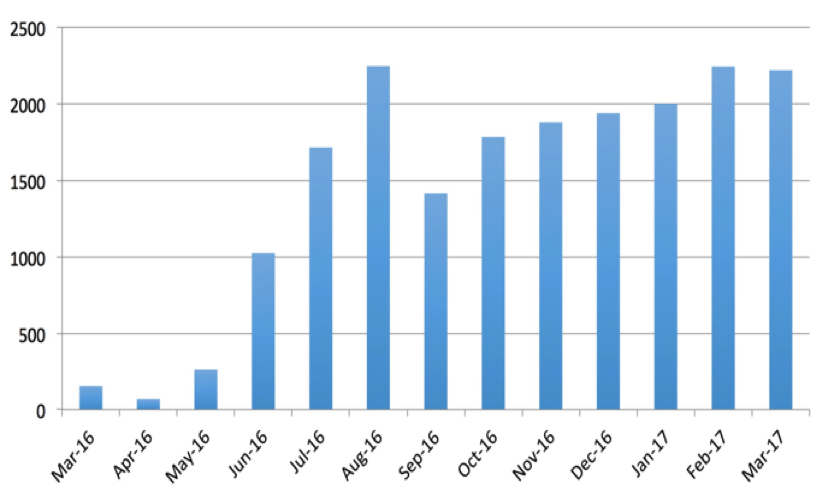
The programme took off in June 2016 and over the following year, held approximately 2,000 meetings every month. We extended this large UPHSSP-led accountability initiative into selected villages in the neighbouring districts of Sultanpur and Fatehpur to facilitate a more rigorous evaluation of programme impacts and mechanisms.
 We randomly assigned 120 Gram Panchayats into one of three arms – one that would receive only information; one that would receive information in addition to the GPC-led facilitation; and a control arm that would receive neither. In the first, we visited each household to provide information about the state of health and health services in their village (compiled from household surveys we completed in the preceding months). Households were also informed about their rights and entitlements, and responsibilities of VHSNCs. Households in the second arm received information in addition to the GPC-led facilitation, and were encouraged to attend VHSNC meetings.
We randomly assigned 120 Gram Panchayats into one of three arms – one that would receive only information; one that would receive information in addition to the GPC-led facilitation; and a control arm that would receive neither. In the first, we visited each household to provide information about the state of health and health services in their village (compiled from household surveys we completed in the preceding months). Households were also informed about their rights and entitlements, and responsibilities of VHSNCs. Households in the second arm received information in addition to the GPC-led facilitation, and were encouraged to attend VHSNC meetings.
After a year of GPC-led facilitation, the UPHSSP-SIRD contract came to a close and we conducted a follow-up with households in these 120 villages. Using anthropometric data collected from 5236 children from 4443 households, we compare outcomes between households in villages that received the GPC-led facilitation in addition to information, and those that received only information, to the households in villages that received neither intervention. Recall that our results come from a randomized controlled experiment. Hence, we are able to estimate the effect caused by the intervention using statistical regression methods that also account for other household and village level characteristics.
Results
The figure below shows impacts on key outcomes in the study. The dots in the figure are the estimated effects and whiskers are the 95 per cent confidence intervals – an interval that crosses the zero line suggests the chance that there was actually no effect.
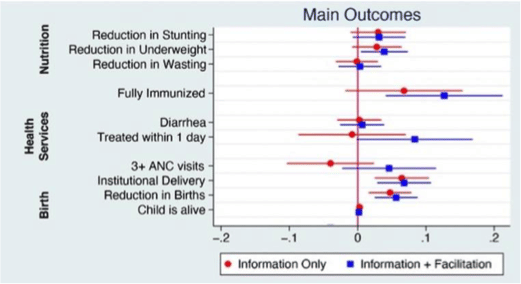 The interventions had large effects on immunisation rates and on facility deliveries. In areas with GPC-led facilitation combined with information, full immunisation rates among young children rose by nearly 13 percentage points — from 43.9 per cent to 56.6 per cent. The increase in information-only arms was smaller and did not represent a statistically significant improvement compared to the control group in the study. Both forms of the social accountability interventions led to significant increases in rates of institutional delivery – increases of nearly 8 percentage points. The interventions also reduced childhood stunting and underweight by about 8 per cent, but these were not precise, as seen with the whiskers crossing the zero line. There were no effects on child mortality or on measures related to childhood diarrhea.
The interventions had large effects on immunisation rates and on facility deliveries. In areas with GPC-led facilitation combined with information, full immunisation rates among young children rose by nearly 13 percentage points — from 43.9 per cent to 56.6 per cent. The increase in information-only arms was smaller and did not represent a statistically significant improvement compared to the control group in the study. Both forms of the social accountability interventions led to significant increases in rates of institutional delivery – increases of nearly 8 percentage points. The interventions also reduced childhood stunting and underweight by about 8 per cent, but these were not precise, as seen with the whiskers crossing the zero line. There were no effects on child mortality or on measures related to childhood diarrhea.
Also read: India has too many tiny farms in agriculture and tiny firms in industry. That’s a problem
Implications on child development
What lessons about governance and health service delivery can we draw from this study? Combining information provision with facilitated community meetings in places like rural Uttar Pradesh can lead to large improvements in childhood immunisation rates and birth outcomes, which in turn will have dramatic long-term implications for child development.
An important feature of our study was that the interventions were implemented by the state government in a manner that is scalable across Uttar Pradesh. Another notable factor was that it took an unusual level of commitment and engagement from the state government to undertake and implement an innovative accountability program. Sadly, due to budget limitations, the programme was discontinued, suggesting that such commitment can be hard to replicate or sustain despite strong engagement and use of evidence.
Our research suggests that information is powerful and that it can be even more impactful when combined with appropriately designed and integrated facilitation mechanisms to empower communities and make public officials more accountable. The governments of Uttar Pradesh and other states in India should take our findings into account as they develop future programmes to promote community monitoring and increase accountability.
Manoj Mohanan is Associate Professor of Public Policy, Economics and Global Health at Duke University. Vikram Rajan is Sr. Health Specialist at the World Bank. Kendal Swanson is a PhD student in Public Policy at Duke University. Harsha Thirumurthy is Associate Professor of Medical Ethics and Health Policy at University of Pennsylvania. Views are personal.
Yes, a Homeopath prescribing Arsenica Alba and an Ayurvedic prescribing Cow Urine for COVID-19 need to be held accountable when the patient dies.
Can we also hold AYUSH ministers accountable whenever they recklessly propagate false information in times of Pandemic?
Indians love beating health care workers
Los Angeles Times, “Choir Practice turns fatal. Airborne Coronaviurs strongly suspected.” March 29. This confirms March 17 study put out by the New England Journal of Medicine that the virus is viable and infectious for 3 hours under laboratory conditions.
This changes everything. I hope Print understands its significance. There aren’t much ventilators or ICU beds to go around. Instead of trying to frame agenda and play petty politics, inform people of the real danger. Do something useful for change.