



Prime Minister Narendra Modi, in his second address to the nation on Covid-19 response, announced a 21-day nationwide lockdown for all citizens, requesting everyone to observe social distancing by staying home – and not crossing the Laxmanrekha to step outside.
The Prime Minister also announced a general economic package of Rs 15,000 crore to be utilised in scaling-up medical requirements for testing, personal protective equipment, ventilators, ICU beds etc.
A prolonged lockdown, in words of the Prime Minister, is perhaps the “only way” available to “flatten the curve” and minimise the incidence of infected cases across states.
While many (including us) would have expected the Prime Minister to announce more targeted measures of economic relief -and reassurance to many of the vulnerable socioeconomic groups and firms, which seemed overdue, his address didn’t include any of these steps. Nor did it highlight any detailed measures to increase the state-capacity and public provisioning of medical services (including increase in number of medical staff, doctors, nurses, pathologists, paramedics).
Also read: More financial services, manufacturing units exempted from coronavirus lockdown
Critical questions
Two critical questions emerge at this point.
Is India’s healthcare-system capable of responding to a pandemic outbreak in days to come?
The Prime Minister clearly affirmed that countries with even the most sophisticated healthcare systems (US, Italy, France etc.) were not able to respond to the outbreak thus far.
And, if this also applies to India, a second question that still stands out is: What are the key economic and institutional measures that the Union government must take to go beyond its announcement of a 21-day complete lockdown, in fighting this virulent disease?
Any comprehensive financial support package would require a large scale two-pronged, synchronized fiscal strategy between the Union and state governments. One, in terms of providing immediate relief to vulnerable groups in form of unemployment insurance, paid leaves, direct transfers to contract and daily-wage workers (who have lost their jobs now), public provisioning of essential nutritional requirements, among others, as part of a distinct/separate financial package. Implementation remains always difficult but atleast a targeted intervention in these areas, is vital.
And second, something the Rs 15,000 crore allocative announcement signals to represent, is to assign more financial allocations for meeting urgent requirements of testing, medical equipment and health-facilities across states. One might argue that it would be better to have this particular nature of allocation financed through a separate, time-bound, special purpose government vehicle functioning in form of a National Health Finance Corporation (NHFC), explained later in detail.
A comprehensive strategy like this may help provide immediate support (and reassurance) to the poor and those at the bottom of the socioeconomic pyramid, and also help give immediate infrastructural support to overworked medical staff in an underfunded public health system through a centralised one-stop shop NHFC financial model.
Why is this needed in India’s grossly underfunded and asymmetric healthcare landscape?
India reports one of the lowest public healthcare spending in proportion to its GDP among the SAARC nations.
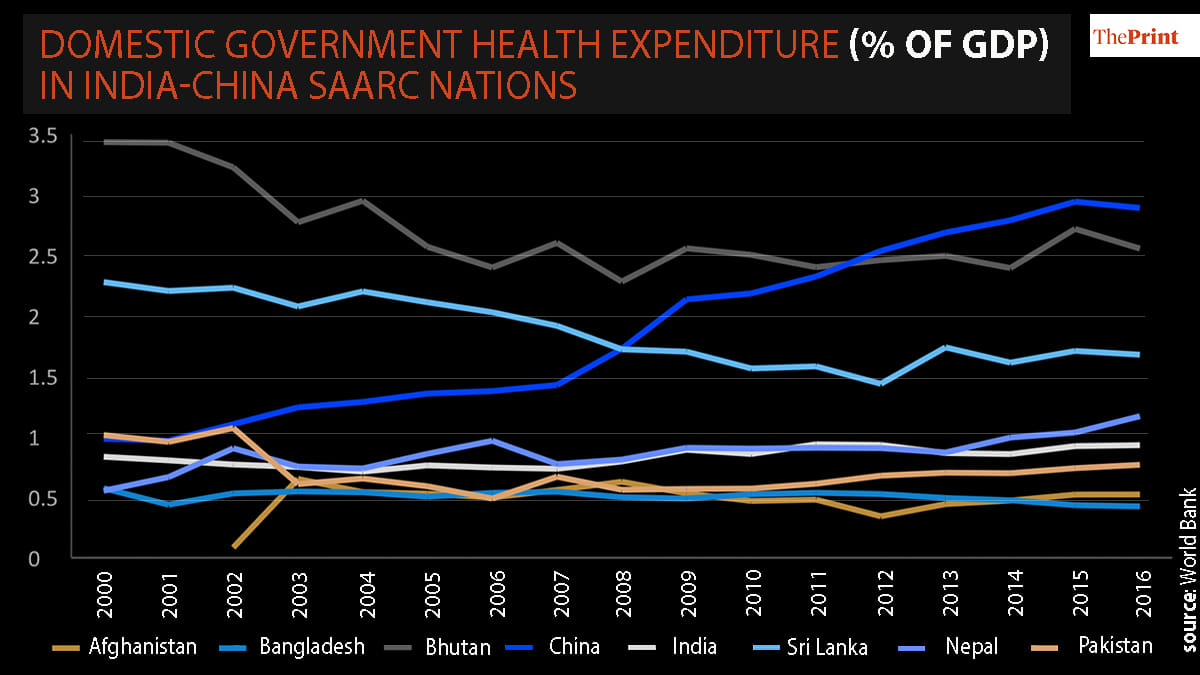
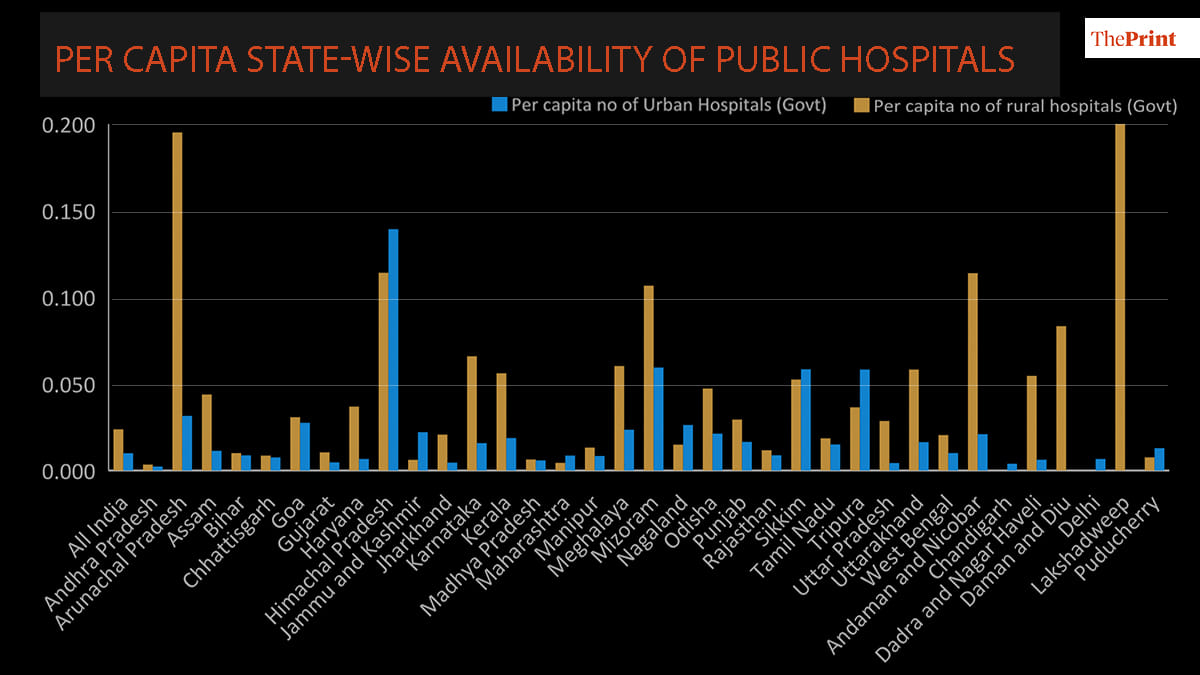
The asymmetric, privatised nature of India’s healthcare system also suffers from wide state-level, urban-rural disparities, which makes it extremely difficult to have any uniform plan in response to a large-scale health crisis, especially in a pandemic outbreak like now.
The Prime Minister was right in asking the private sector to step in and support all government healthcare system. One way to do so is by perhaps by enabling more private production of healthcare equipment (testing kits, masks, personal protective equipment, ventilators etc.) and use public (state) provisioning to supply these across states and also include private diagnostic labs and hospitals to subsidise their services in accommodating testing and treatment for all.
Also read: Mahabharata war won in 18 days, but fight against coronavirus will take 21 days, says Modi
Indians spending on health
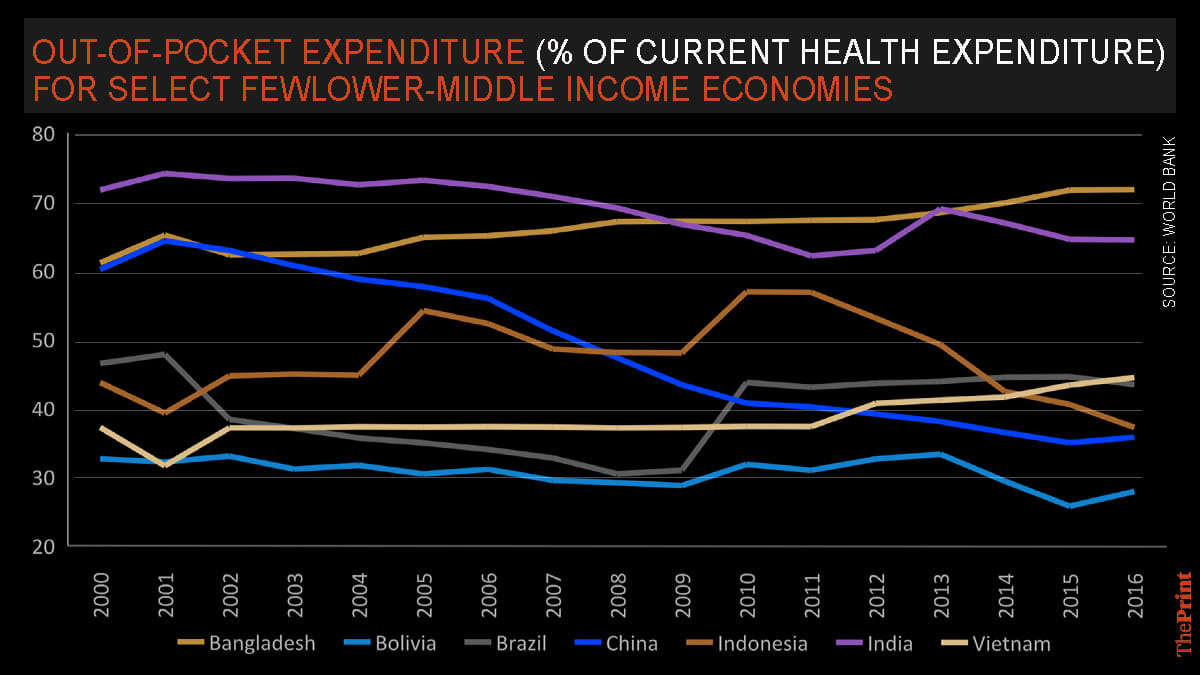
From the citizenry’s perspective, in a system where private healthcare proportion of spending is much higher than the government across states and in urban spaces, the share of out of pocket spending on overall medical cost and expenses by Indians remains higher than most the other developing countries.
Over the last decade and more, from a high out of pocket expenditure, most Indians, have financed their medical expenses through their respective household income or savings. Many of those at the bottom of the socio-economic pyramid, would find it extremely difficult to afford the Rs 4,500 Covid-19 test fee (that private labs have been notified to charge).
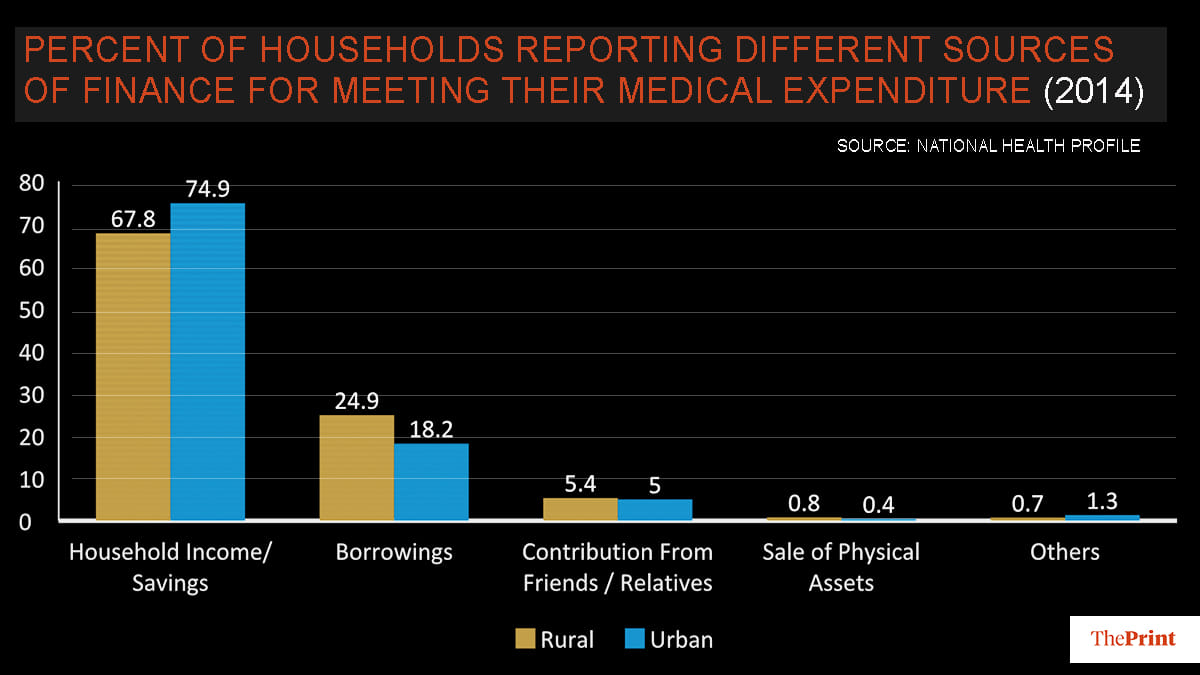
How can people in rural communities, migrant and daily-wage workers be expected to undertake high medical costs at a time when mobility is restricted and most have lost their jobs after a complete lockdown is in place. Immediate direct cash transfers would be needed to not only help them have enough disposable incomes to finance essential costs/expenses but would also require subsidised rationing of public essentials (nutrition, healthcare, shelter).
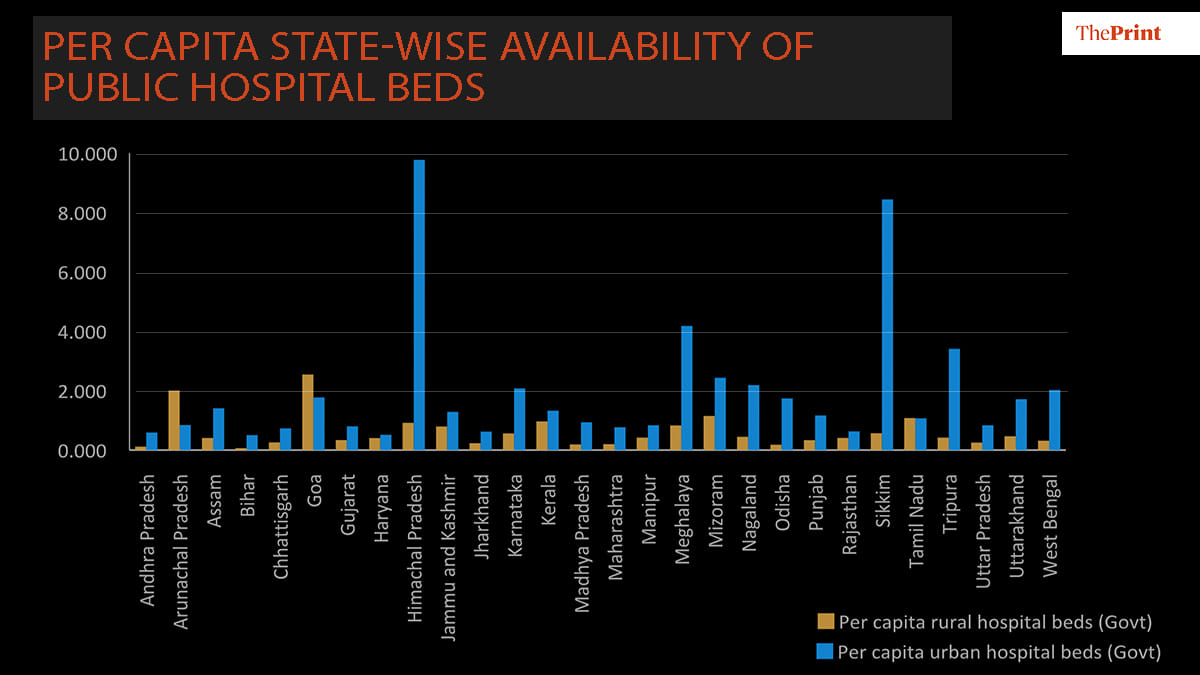
Most states have also seen a significant decline in number of public health facilities over the last decade, except for states like Andhra Pradesh, Jharkhand and Bihar which have increased sub-centres like PHCs, CHCs. There is a massive state-level variation in the number of public hospital beds per capita available within urban-rural areas.
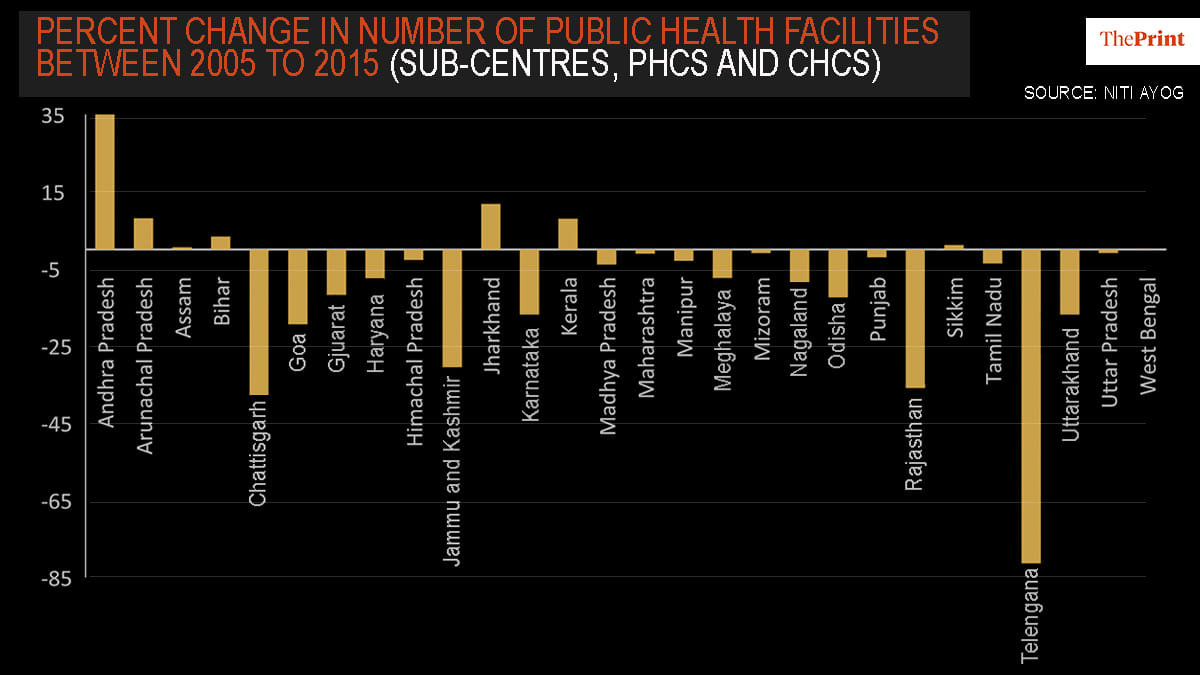
The Union government must ensure that all states have enough make-shift public health facilities and hospital arrangements to treat and accommodate for diagnosed positive cases, while ensuring segregation of the infected population group from the non-symptomatic group, like in China, South Korea, Singapore and Taiwan.
Also read: Delhi, Gurugram police promise ‘seamless’ delivery from Amazon, Big Basket, Zomato, Flipkart
Public-private strategy
A comprehensive public-private strategy is still needed to be in-effect that can channelise all possible economic resources in building up infrastructural capacity for hospitals and medical personnel across states. The Prime Minister did mention in his address how he has urged all states to put their fiscal resources towards healthcare as top priority, but states, as seen in case of Kerala, Maharashtra, without the Centre’s direct support may fiscally stretch out, or worse, exhaust their medical capacities (Isolation beds, ICU beds) soon, if cases rise exponentially.
To catalyse a more robust Union-state partnership, the existing federal nature of bureaucratic channels may also make decision-making processes of such nature more difficult in a crisis response.
Also read: Modi announced it last Thursday but Covid-19 economic task force nowhere in sight
The SPV we need
In a public-health emergency like this, it might be worth having a time-bound, government-controlled special purpose vehicle (SPV) at the centre to coordinate a healthcare action plan against any epidemic outbreak.
Institutionally, the Union government, through its emergency financial powers, can establish a one stop-shop, time-bound special purpose vehicle in the form of a National Health Finance Corporation (NHFC).
The NHFC, earlier proposed by American economic historian Barry Eichengreen, can function as a remodelled version of the Reconstruction Finance Corporation, created in response to the Great Depression in the US to support plans under the New Deal (under Roosevelt) and helped stabilise the banking sector under the Hoover Administration (1932).
In the Indian context, the NHFC can help coordinate with all central, state and local government public (PHCs, CHCs) and private health facilities, scale up gaps in medical infrastructural requirements across cities and rural areas through a centralised channel.
With exclusive financial powers granted from the Union government, the institution can also help ensure a swift transfer of capital and medical resources for transport to states with large-infected populations. As of now states like Maharashtra, Kerala could to be prioritised. The SPV could also provide essential units of ventilators, respirators, masks and other personal protective equipment for medical staff and doctors (to limit their own exposure).
Creation of such a government-owned SPV can be financed in the short to medium term through a special contingency fund sourced from a temporal wealth tax (say, 2-3 per cent) on the top 1 per cent wealth group, along with an encouragement of other voluntary mechanisms and (tax-free) contributions from the most wealthy to generate enough private capital for pooling and crowding-in resources.
Also read: Chidambaram proposes cash transfers to urban, rural poor to help them during lockdown
The economic fallout
What about the overall economic fallout from the crisis?
The Prime Minister failed to provide any financial support that is required in addressing the economic fallout of this crisis or in supplementing some basic fiscal transfers provided to to the most vulnerable by state governments like Delhi, Kerala, West Bengal, Punjab, Rajasthan.
A 21-day lockdown means an unemployment shock of a kind that has never been witnessed in India’s post-independent economic history. India was already experiencing a structural downturn where unemployment was at a 45-year high.
For worse, shortage of essential supplies coupled with restricted mobility for service providers and lack of transport may result in more instances of social unrest. Police brutality along with an increase in food prices will make it all the more difficult for lower-middle income (and poor) groups to get access to basic essentials (as discussed here).
From a supply-side perspective, many businesses, service providers included, may go out of business over a long lockdown period like this.
To address these critical economic concerns, one would have expected a comprehensive stimulus plan to compliment any national-lockdown strategy. And to work this out, even now, money-taps should be wide-opened from both monetary and fiscal channels for preparing for these large demand-and-supply side shocks.
The Reserve Bank in synchronized effort with Union government can print more money and use available monetary policy tools to provide greater liquidity to institutions like NHFC, along with the creation of a direct credit-channel through commercial banks to help most affected small-medium-large scale businesses across sectors (tourism, aviation, FMCG etc.).
This can enable most affected firms to not let go of contract workers in weeks to come and later restore supply-capacity once the sudden-stop effect on business (imposed from the current lockdown) gets off. This will also help calm the debt and equity financial markets (currently tanking).
Fiscal support measures for affected companies could include an exemption from goods and services tax and direct tax payments for at least the next 1-2 years.
A lockdown-dependent pandemic response reflects an action-plan that is out of context to India’s existing social and economic realities. Unlike developed, organized economies, where lockdowns can be managed over longer periods by ensuring transfers to people’s accounts-and firms, India has more than 90 per cent of its workforce in areas of unorganised, informal sector.
A laissez-faire economic response of letting things be, as seen so far, may just make India enter into a long cycle of a great depression, that, in both, scale and form would be far worse than the Great Depression experienced by the US and Europe in late 1920s and early 1930s.
Deepanshu Mohan is Associate Professor and Director, Centre for New Economics Studies, O.P. Jindal Global University. Ayona Bhattacharjee is an Assistant Professor at International Management Institute (IMI), New Delhi. Views are personal.
If a professor is using colorful graphs, one can safely assume that this professor is an in sane librandu.
These professors have nothing else to do except break their heads with the stone and then accuse the government for injuries.
Sale mar ja kue me kud ke