



New Delhi: A couple opting for in-vitro fertilisation (IVF) in India can now find out which of their embryos carries the risk of heart disease, diabetes or Alzheimer’s—years or decades before any such condition could manifest.
It won’t be a diagnosis. It will be a probability.
That number—called the polygenic risk score (PRS), arrived at after analysing genetic variations in an embryo’s DNA with the help of artificial intelligence—marks a significant transformation under way in India’s fertility industry.
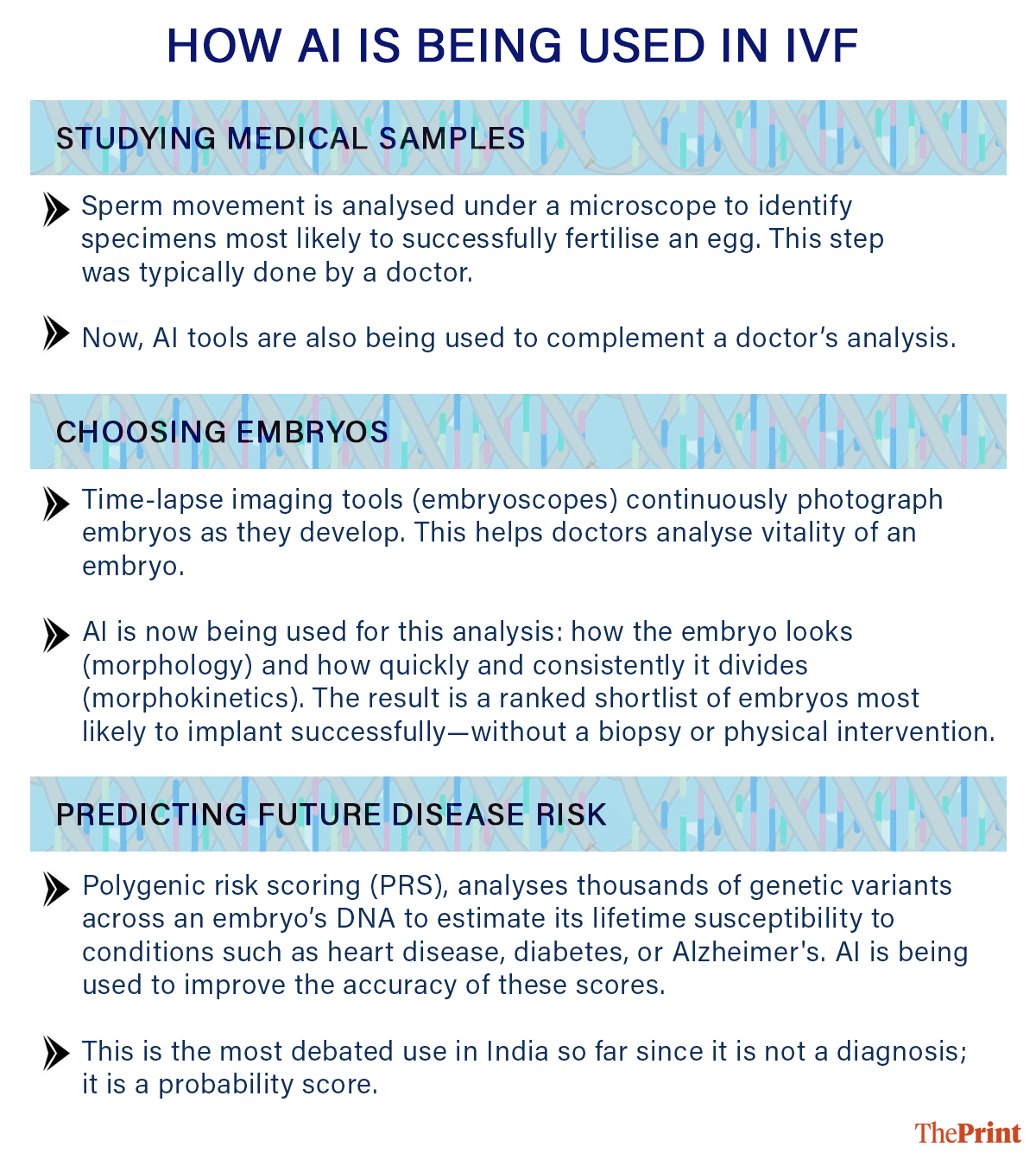
As of early 2026, at least six major fertility chains and several regional clinics across the country have integrated AI tools into their IVF services. The tools fall broadly into two categories: those that analyse sperm and/or embryo images to predict implantation success, and those that study DNA to estimate a child’s susceptibility to disease.
New York-based startup Nucleus Genomics in March partnered with Indira IVF—India’s largest fertility provider founded in Rajasthan’s Udaipur—to offer embryo-level polygenic screening. Indira IVF operates around 160 clinics nationwide, and says it performs nearly 42,000 IVF cycles a year.
Then, Delhi-based Gaudium IVF tied up with IVF 2.0, a UK-headquartered embryology organisation, to deploy two image-based tools—ERICA (Embryo Ranking Intelligent Classification Assistant) and SiD (Sperm Identification Device).
Nova IVF Fertility, also Delhi-based, rolled out Vita Embryo, an AI embryo assessment system by South Korea’s Kai Health, across 120 clinics in 65 Indian cities.
The commercial logic is clear. India’s IVF market was valued at $961 million in 2024 and was projected to reach $1.49 billion by 2030, driven by delayed parenthood, rising infertility rates, and a middle class increasingly willing to pay out of pocket, according to market research firm Techsci Research. An estimated 27.5 million Indian couples experience infertility, the 2025 State of World Population Report by the United Nations noted.
The clinical, ethical, and legal questions raised by this expansion within the fertility industry—particularly around DNA-based screening—are considerably less settled.
Also Read: Economic Survey flags digital addiction risk for India’s youth, advocates for balance over bans
How AI helps embryo selection
When a couple undergoes IVF, doctors stimulate the ovaries to produce multiple eggs, fertilise them in a laboratory, and then determine which embryo to transfer to the uterus. Not all embryos are viable—and identifying those most likely to result in a successful pregnancy remains one of fertility medicine’s central challenges.
Dr Juhi Bharti, additional professor in the Department of Obstetrics and Gynaecology at the All India Institute of Medical Sciences (AIIMS), New Delhi, said AI is now being used across stages—from embryo selection and predictive modelling to sperm assessment—to improve IVF outcomes.
“In embryo selection, we traditionally assess embryos under a microscope or use genetic testing. But AI can evaluate parameters that go beyond normal human capabilities,” she said.
One of the key tools is time-lapse imaging, which continuously captures images of developing embryos. These systems analyse both morphology—how the embryo looks—and morphokinetics, or how quickly it grows and divides. By combining these inputs with algorithmic models, AI can help identify which embryo has the highest likelihood of success.
“Instead of going for invasive genetic analysis, which is not always available and can also lead to embryo loss, this is a non-invasive way of interpretation. The devices used for this use time-lapse technology—these are the tools we use to assess which is the best embryo,” Dr Bharti explained.
ERICA, the system deployed by Gaudium IVF this April, analyses embryo images against large historical datasets to rank those most likely to implant. SiD performs the equivalent function for sperm, examining movement patterns under a microscope to identify specimens most likely to successfully fertilise an egg.
Dr Manika Khanna, founder and managing director of Gaudium IVF, was precise about the tools’ scope. “It tells you how healthy the embryo is going to be in terms of implanting inside the womb,” she said.
“These tools do not help in making green-eyed, fairer babies. They just can’t. They can just tell you, out of what you’ve already created, which embryo is most likely to give you a healthy pregnancy,” Dr Khanna added.
Gaudium is currently absorbing the cost of ERICA rather than passing it to patients. “We are aiming at getting more and more pregnancies. We do not wish to pass the cost burden to the patient because more pregnancies, more word of mouth, more business,” Dr Khanna said.
What polygenic risk scoring measures
The importance of accurate selection of embryo compounds with age. A healthy human cell contains 46 chromosomes—23 pairs carrying the body’s genetic instructions. Even a small imbalance can render an embryo non-viable, leading to failed implantation or miscarriage.
“The problem worsens sharply with age. Between 30 and 35, around 60 percent of embryos may be chromosomally normal. By 42, that drops to about 20-25 percent,” Dr Kshitiz Murdia, CEO of Indira IVF, said.
He added, “The older the patient, the harder it becomes to find a viable embryo—and the more critical it is to identify the right one quickly.”
The established tools for addressing this are PGT-A (Preimplantation Genetic Testing for Aneuploidy), which checks whether an embryo has the correct number of chromosomes— identifying abnormalities linked to miscarriage or conditions such as Down syndrome—and PGT-M (Preimplantation Genetic Testing for Monogenic disorders), which screens for specific inherited single-gene conditions such as thalassaemia and sickle cell disease. Both require an embryo biopsy, where a small group of cells is extracted and analysed in a laboratory.
What is now emerging—and remains considerably more debated—is a third layer: polygenic risk scoring.
Unlike earlier methods, which look for discrete genetic defects, PRS estimates the probability of developing complex diseases driven not by one gene but by tiny variations spread across an individual’s DNA.
Each genetic variant is assigned a weight based on how strongly it has been associated with a given condition in large population studies. Combined, these weights produce a single score that positions an individual on a risk continuum. The score is not a diagnosis; it indicates where a person sits relative to the broader population.
The idea is not new. PRS was first developed around 2007 as a research methodology. Its clinical application in IVF—scoring embryos before implantation—began around 2019.
Kian Sadeghi, founder and CEO of Nucleus Genomics, explained the process. “We analyse genetic data from millions of people, including strong representation from South Asian populations,” he said.
“By comparing individuals who have a disease with those who do not—and adjusting for factors like age, sex, and ancestry—we can identify genetic variants that are more common in those affected,” he said.
“These markers are then combined algorithmically to generate a score, which places an embryo on a risk curve relative to the general population for conditions such as Alzheimer’s, breast cancer, or Type 2 diabetes,” he added.
The basis for this study rests on a biological constant. “An embryo’s DNA is the same as an adult’s DNA. Since DNA does not change over time, it can be used to estimate the likelihood of developing certain diseases later in life,” he said.
Indira IVF’s Murdia said this approach to using AI was selective and begins with the parents, not the embryos.
“We are not offering this to every couple who is going through IVF,” he said. Both partners are first screened via buccal swabs to assess whether they carry a higher likelihood of conditions such as hypertension, cancer, or Alzheimer’s. Only if a significant predisposition is identified does the process advance to embryo-level testing.
A standard IVF cycle at Indira IVF costs between Rs 1.8 lakh and Rs 2.5 lakh. Adding expanded genomic screening brings costs up by another Rs 2–3 lakh per round. For many Indian families, IVF alone is already a financial stretch.
The limits of a number
Polygenic risk scores are, by design, probabilistic, and not an absolute science.
Sadeghi acknowledged this, and said, “No genetics company could ever say we can perfectly predict disease. For example, something like skin cancer, there’s a smaller genetic component, but there’s a very large environmental component.”
For conditions such as heart disease or Type 2 diabetes, he argued, the genetic contribution can reach up to 50 percent. The other half—diet, exercise, chance—lies beyond the model’s reach.
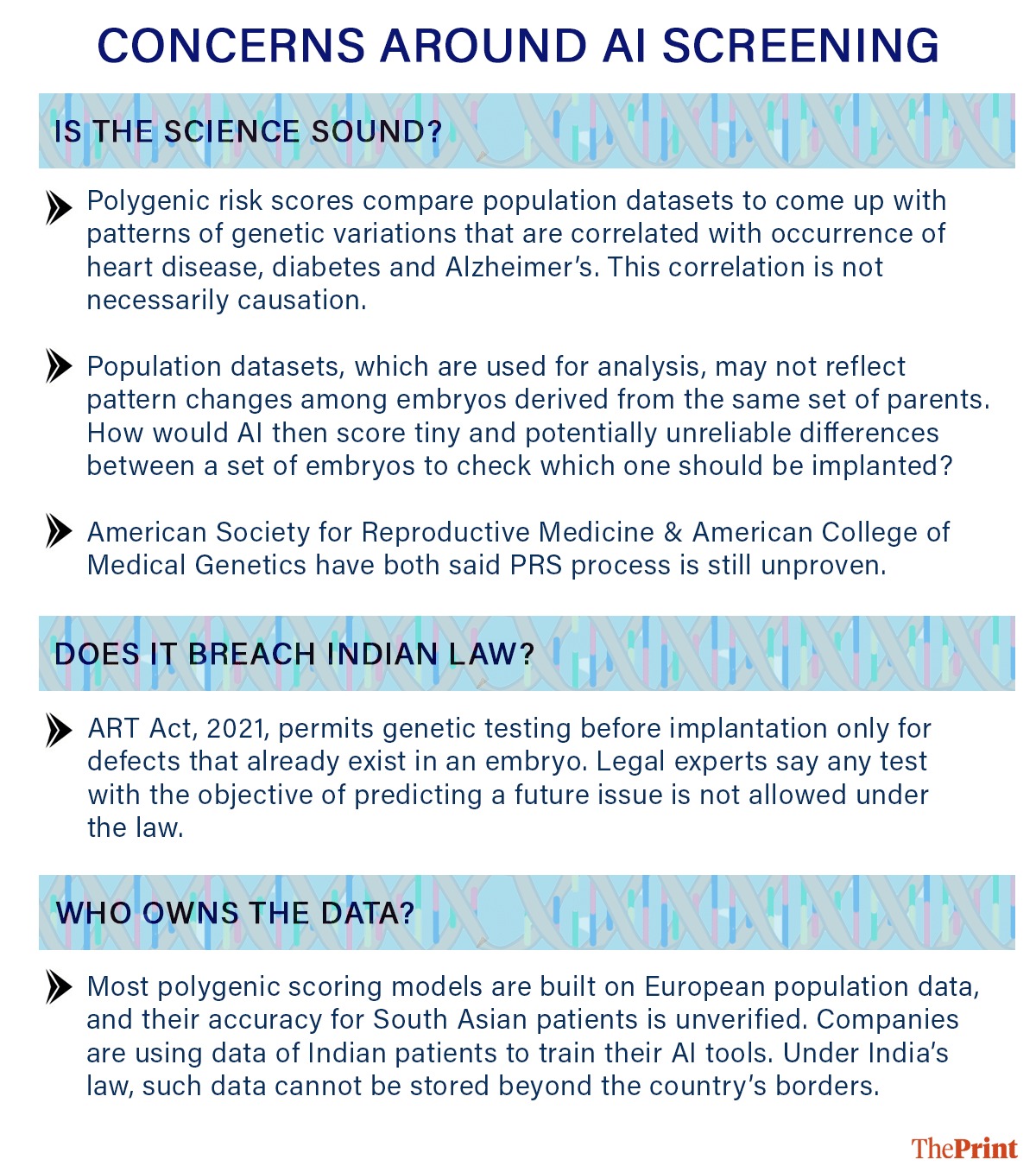
Scientific scepticism about PRS runs deeper than the familiar uncertainty around probabilistic statistics. There is a structural problem specific to applying these scores in IVF: they are built by comparing genetic patterns of unrelated individuals across a broad population.
When the same scores are applied to embryos from one couple—whose genomes are both derived from the same two parents—the variation between them is far smaller than between strangers. Because every embryo’s genome is a combination of those two parents’ genomes, the scores become less reliable precisely where they are needed most: to distinguish between embryos from the same couple.
A 2021 paper in the New England Journal of Medicine, titled ‘Problems with Using Polygenic Scores to Select Embryos’, set this out in mathematical terms.
Professional opinion has since hardened in the same direction. In December 2025, the American Society for Reproductive Medicine published a joint report concluding that polygenic embryo screening is not ready for clinical practice and should not be offered as a reproductive service, citing predictive uncertainties and substantial ethical considerations.
The American College of Medical Genetics and Genomics had reached a similar conclusion in 2024, stating that the clinical utility of such testing to reduce disease burden remains unproven.
Dr Sabine Kapasi, a public health expert and founder of Delhi-based health-tech company Ropan Healthcare, said, “The point is I can give you a risk score based on the parents and their lifestyle itself, and that would probably be almost as accurate.”
Kapasi, who has worked with global health agencies, including the World Health Organization (WHO), emphasised that such tools rely on patterns in data, not proven cause-and-effect relationships. “Technologies like polygenic risk scores rely on large-scale population and familial data to generate probabilistic risk estimates. These are based on statistical associations rather than direct causation. While certain genetic markers are well validated, many signals, particularly in polygenic models, still require stronger evidence to establish consistent clinical utility across populations,” she said.
Kapasi also questioned the clinical usefulness of such testing. “The key question is whether this meaningfully enables early risk reduction or informs clinical decisions. Otherwise, there is a risk of adding complexity without a clear benefit to patient care. That, to me, is the real issue here.”
Dr Hrishikesh Pai, founder and medical director of Bloom IVF—which operates across Mumbai, Delhi, and Gurugram and deploys Life Whisperer, an AI embryo assessment tool by Australian medical imaging company Presagen—was equally measured.
“At present, it (PRS) should be viewed as investigational rather than established clinical standard care. It must not replace conventional embryo selection based on embryo quality, chromosomal normality, and sound IVF principles. Strong ethical counselling and transparency are essential,” he said.
Law, data & regulatory concerns
India’s Assisted Reproductive Technology (ART) Act, 2021, allows preimplantation genetic testing only for known, pre-existing, heritable or genetic conditions. Experts say the legislation was designed with single-gene disorders (where mutation in one gene can lead to disorders such as sickle cell anaemia and Huntington’s disease) in mind.
Indira IVF CEO Murdia maintained that the PRS approach was consistent with the Act’s provisions.
But Biplab Lenin, a healthcare and life sciences lawyer and Partner at Cyril Amarchand Mangaldas, speaking in general terms about the legal framework without reference to any specific parties, identified a tension.
“Under Section 25 (of ART), preimplantation genetic testing has been defined to mean techniques used to identify genetic defects in embryos. Therefore, the defect must be present at the time of testing, and this does not include predictions based on statistical probability,” he said.
He added that while an argument could be made that polygenic predisposition qualifies as a heritable condition, “At best, the testing may be carried out for a known genetic abnormality in patients to confirm whether the embryo also has that abnormality. The objective of the test cannot be to predict the possibility of the same issue developing in the future.”
Radhika Thapar Bahl, a Delhi-based advocate and founder of Fertility Law Care, described as one of India’s leading practitioners in ART law, drew the same line. “Only in cases where there is a pre-existing condition, and that too not for gender detection, does the law allow you to go for PGT-A or PGD testing.”
Bahl also raised the question of what happens when AI and a doctor’s judgement diverge. “Suppose the embryologist picks a certain embryo and the AI picks the other one. Who decides? That information must be given in clear transparency,” she said, adding that patients who are not fully informed of a technology’s limitations before treatment begins cannot pursue negligence or consumer litigation after the fact.
Murdia acknowledged the communication challenge. “The data is complex, no doubt. But the final output report that comes is very simple to understand, even for the doctors and for the patients,” he said.
Both legal experts also raised a concern that runs beneath the compliance debate: the data on which polygenic models are constructed. Most genome-wide association studies used to build these scores were drawn predominantly from European populations, raising questions about accuracy when applied to South Asian patients.
Gaudium confirmed that its own historical patient records—including embryo images—are being used to fine-tune ERICA for the Indian clinical context.
Lenin flagged the longer-term implications of such a use. “This aspect (using data of Indian patients) would require detailed analysis as the law is developing. The Digital Personal Data Protection (DPDP) Act and Rules are new. AI and data-related aspects are evolving. Consent would play a vital role,” he said.
Murdia, of Indira IVF, asserted that all rules were being followed. “The regulations say the data cannot go out of the country. Nothing goes out from a compliance point of view,” he said.
(Edited by Prerna Madan)