





This week, my father and siblings had an Easter like no other. We held an online ‘HouseParty’ with the whole family, which was a chaotic but fun thing to do, and my sister’s children went Easter Egg hunting in my parents’ garden. We were hoping that with the return of warm weather, we could see each other again in person by the summer. But my father threw some cold water on that hope, though he did give us a solid explanation why. Have a read below.
— Peter Vanham
Dear Nele, Johan and Peter
We just had a beautiful Easter weekend, with great weather and a longing to go outside and meet family and friends. In our case, we found again a creative solution for the grandchildren to come by: on Sunday morning, we hid Easter eggs in the garden, and in the afternoon, the children came to look for them, while we looked from a safe distance. It’s not the same as before, but for both the children and for us, it was a nice experience.
I think, we’ll have to get creative like this for another few months, and certainly through the summer. As you know, we will only have a lasting solution when we get to herd immunity, and the safest way to achieve it is by developing a coronavirus vaccine. We would all want this vaccine to be there sooner rather than later, but my assessment is that a vaccine will likely not be widely available until 2021, and possibly later. In the meanwhile, we have to hope for an effective drug by fall. To help you understand this, I thought I’d explain the various phases and techniques to get to a vaccine.
I’ll try to make this as straightforward as possible, but it does require you to sit down and read attentively. In return, I’ll summarise some basic insights of decades of virology research and development into an understandable text. If after reading this letter you still want to read more about the specific case of a SARS-CoV2 vaccine (the novel coronavirus’ scientific name), I recommend this excellent paper by Fatima Amanat and Florian Krammer — SARS-CoV-2 Vaccines: Status Report. Now, let’s start!
Also read: We must not return to work for now. Covid’s not over yet, says a virologist in letter to son
The vaccine candidates
The main distinction you need to understand is between the initial development of vaccine candidates and their pre-clinical (non-human) testing, and the subsequent various phases of human testing, followed by production, distribution, and administration. For all but three vaccine candidates for SARS-CoV-2, we are still in the non-human phase, and many candidates may be ‘stuck’ in there for weeks, months, or even years, possibly not getting through at all. It’s only when they get through the initial phase that candidates really get to the start of the ‘race to the vaccine’.
Compare it, if you will, to the audition rounds of America’s Got Talent, versus the live shows. To extend that analogy a bit, consider that ‘Vaccine’s Got Talent’ welcomes candidates using different methods. But instead of singing, dancing, stand-up, and magic tricks, vaccine candidates can come from six different categories: ‘live attenuated’ or ‘inactivated’ virus vaccines, ‘recombinant protein’ vaccines, or ‘DNA’, ‘RNA’ or ‘vectored’ vaccines. Let’s look at those a bit more in detail.
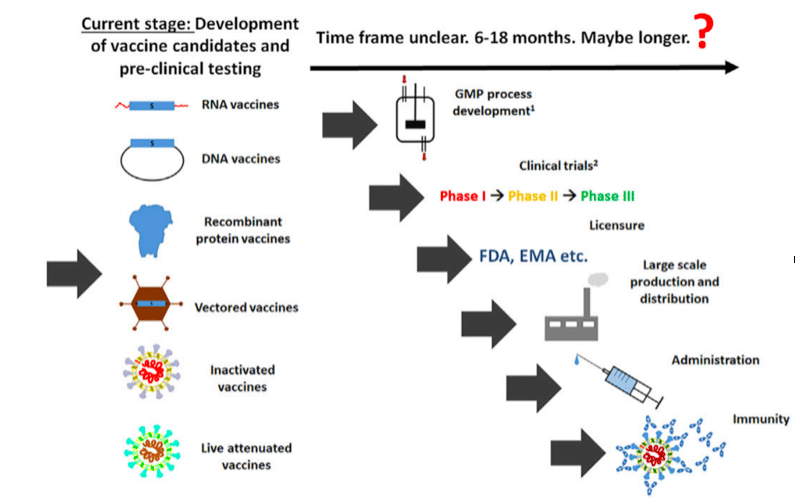
Source: Amanat and Krammer, SARS-CoV-2 Vaccines: Status Report, Immunity (2020)
Live attenuated and inactivated vaccines are easy to make. They are the ‘classic vaccines’ that we know from the measles and the flu. You isolate a little bit of virus, weaken or ‘inactivate’ it, and then inject it into a human being in a portion that is small enough to trigger a reaction from your body. Production capacity for such vaccines exists since the 1950s. If such a vaccine would work, you can go to market relatively quickly.
We also have experience with recombinant protein vaccines: this method is used, for example, for the human papillomavirus that causes cervical cancer, or for the hepatitis B vaccine. The latter vaccine exists since the 1980s — I was vaccinated against Hepatitis B in the 1980s in Belgium — and that makes them ‘second generation’ vaccines. This type of vaccine doesn’t use the virus itself, but the proteins on the outside of it. In the case of the coronavirus, these vaccines would use the ‘spikes of the crown’ of the virus, to give you a visual image. It is this ‘spike’ or ‘crown’ that the virus uses to attach itself to our cells. If you inject a vaccine that will make us produce antibodies to block the protein from attaching itself, then, the virus might not be able to enter our cells.
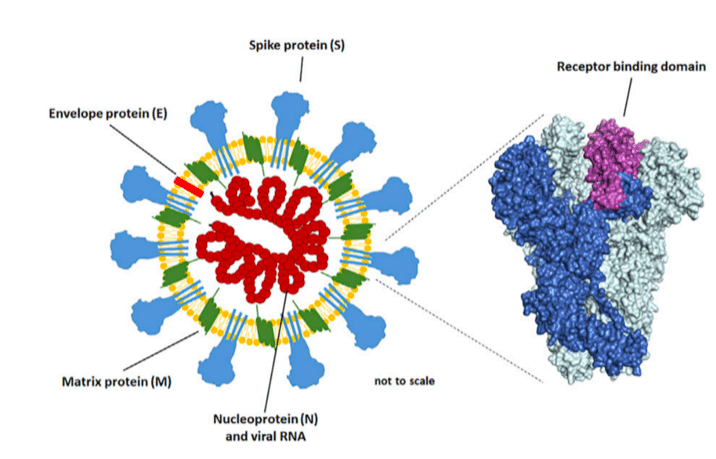
Source: Amanat and Krammer, SARS-CoV-2 Vaccines: Status Report, Immunity (2020)
There is a trick with them: it’s not certain whether human antibodies, elicited against those ‘spike’, ‘surface’ or ‘envelope’ proteins, will protect you from the virus. With HIV, for example, my specialisation, we’ve tried a similar technique for more than 30 years, and we still haven’t found one that works. But for the novel coronavirus, there are good signs it could work: for SARS and MERS, notably, two other coronaviruses, the technique did work in some animal models (though the vaccines weren’t used widely; the virus died before the vaccine was produced for humans). Still, if this technique works, it might take a little longer to set up the industrial production and administration, but it is certainly possible since it’s already in use for papilloma and hepatitis B.
Finally, if one of the above three principles doesn’t work, there are also the DNA, RNA or Vectored vaccines. The principle for all of them is that you take a piece of the genetic coding of the virus, namely one that would trigger your immune system to get alerted, and inject it into the human body, where it is taken up by your cells and they produce the ‘spike protein’ of the virus, against which your immune system will make the antibodies. The technique is new and complicated, and it is part of the ‘third generation’ of vaccines. Only very recently [starting 2015 in trials, and resulting in an approved vaccine in late 2019] ‘viral vector-based’ vaccines were used for the first time in humans — to control the Ebola outbreak in the east of the Democratic Republic of the Congo with apparent success. Clearly, this technique could work, but we have less experience with it, especially to produce and use it at scale. It would, therefore, take more time, but, reportedly, a Chinese company CanSino Biologics is moving such a vaccine already into a preliminary human trial.
Also read: ICMR plans plasma therapy clinical trials in 2 weeks to treat critical Covid-19 cases
The frontrunners
Over all, these techniques combined, there are currently more than 70 vaccine candidates for SARS-CoV-2 being worked on. That may sound like a lot, but bear in mind that the analogy with America’s Got Talent stops here. In the talent show, you’d end up with a winner no matter how many candidates initially signed up. For a new vaccine, however, you can’t be sure if there will be a ‘winner’ at all. You typically need up to 100 vaccine candidates, to get to one winner: one vaccine that works, isn’t toxic, and is easy to produce and administer. The ‘attrition rate’, as we call it, would in such case be 99 per cent.
With all but a few of the candidates we currently have, we would normally first need to run ‘pre-clinical tests’ before we go to the human test phases. In these pre-clinical tests, the vaccine candidate is given to animals that are sensitive to the virus, and that would get sick if they had the virus and developed the disease. That way, you can test not only if the vaccine candidates create antibodies, but whether they protect against the disease infection. For many SARS-CoV-2 vaccine candidates, this pre-clinical trial is the first real hurdle.
An ethical commission, such as the National Institutes of Health in the US, or the Coalition for Epidemics Preparedness Innovation in Switzerland, would have to decide whether the various vaccine candidates have to do testing with animals for safety. If the technique is deemed safe, it will go quickly. If you are more experimental, you’ll need to do a toxicity test with bunnies (which are the typical ‘guinea pigs’) and two other animals, possibly ferrets and hamsters. Such tests can take at least six months in a traditional programme. The vaccine candidate that can’t pass this hurdle, will likely lose the race. It will be a first separation between the more than 70 candidates, though most will pass this test. As I said, three candidate vaccines already cleared this hurdle. They are currently the ‘front-runners’.
Also read: Doctors, IAS officers & a scientist — the 5 women leading India’s fight against Covid-19
The vaccine trial phases
After this phase, the real race to a vaccine starts, with clinical tests on humans. It starts with Phase I, with a few dozen patients, in which you look for the best dose of the vaccine in humans, while observing minimal side effects. It is a safety phase. This Phase I takes various weeks, probably at least two months, because you first need to inject the vaccine to a small number of patients, and wait a week or longer to get results. Then you do the same with another few people, and with a higher dose, and again you wait, and so on, until you get to a target dose you will use for the Phase II and Phase III trials.
Then comes Phase II, with hundreds of patients, to prove the vaccine candidate creates anti-bodies and creates immunity response. This phase uses healthy people who are not necessarily faced with the virus, and it will also take a few months. You probably need to give multiple doses, particularly for the RNA, DNA, vector and recombinant vaccines, because they break down typically before creating strong immunity. You need a 3-4 week interval in between each ‘boost’, and see how the body reacts (that can take a week or two). So for this phase again you need at least two months, and more probably, three months.
Then comes Phase III, where you do a real test for effectiveness, and protective immunity: can the vaccine immunity protect against the infection for the disease? This is the ‘make or break’ phase that will determine whether we have an initial ‘winner’. But the phase will take even longer, as you’ll need to include a lot of people in your trial to know effectiveness: some will get the real vaccine, and others the placebo, and you need to follow them over time to know if there’s a difference in infection between the two groups. That, of course, is a problem: many societies have either strict lockdown measures in place (in much of Europe, the Americas, and the Middle East). Or they have very few infections anymore (in China, Korea, Singapore, and other parts of East Asia).
Either way, this phase will easily last six months, and again, possibly (much) longer, and for the front-runners, will likely start in the fall of 2020. When it takes place, you can see two logical candidates for trial groups: people who live in homes for the elderly, where there are a lot of infections, and people who work in the health sector. The the second group is the most logical, because they are healthy and likely to get exposed to the virus. But you will have to make sure to choose those healthcare workers who haven’t gotten the virus before.
The current coronavirus race
So where are we with the vaccine candidates for the novel coronavirus today? There are 78 candidates. That means there are 78 products, for which an analogue exists for other infectious diseases, that create an immune response there. They are all variants of the six methods I described above, where you can copy-paste what existed for the previous candidate, by taking the DNA code of the new virus, and apply one of the techniques I mentioned. Almost all of the candidates are based on the ‘spike protein’ or ‘crown’, as that protein would fix to the cell, and if you have an anti-body against that, it cannot fix to the cell.
Most of the candidates are still in the non-human development and testing phase. But there is one RNA vaccine currently in Phase I with humans, namely the vaccine of Moderna in Seattle. Another DNA vaccine focusing on the protein is about to start its Phase I, namely that of Inovio in Pennsylvania. One caveat is that these vaccines by themselves may not be strong enough to reach immunity in humans, and may need to be combined with another, recombinant protein vaccine. Hong Kong’s CanSino Biologics says it is about to start a Phase II trial, using the viral vector technique, though no details are known about its Phase I results.
Imagine that any of these frontrunners, or any of the 75 other candidates, successfully make it through Phase III. If they manage to do that, they go to the Approval phase. That is when an institution like the Food and Drug Administration (FDA) in the US, the European Medicines Agency (EMA) in Europe, or the National Medical Products Administration (NMPA) in China, give their ‘blessing’ to the vaccine. Sometimes this phase can take half a year, but in this case, we can assume it will be treated with utmost speed, and then it can be done in a few short weeks.
Then you go to manufacturing, distribution and administration. Those are the economic and logistical aspects. How long this phase lasts, depends on the category that comes through. Here, the frontrunners may lose time, and the laggards may win time: the vaccines using live and attenuated virus, as well as those using the dead virus, have been produced and administrated at large scale before, whereas the others haven’t, at least not at the same scale and speed. For the first-generation vaccines, large pharma companies have the capacity to ramp up their production quickly. But if it is a smaller company, maybe it will take longer. You can look at a few to many months. A good example is the influenza virus. That is being made every year in a couple of months.
Also read: 70 coronavirus vaccines in development, 3 candidates already undergoing human trials: WHO
Distribution of winners
In the end, SARS-CoV2 vaccines will not be realistically available for another 12-18 months. And even then, we must be lucky every step of the way.
Take the example of H1N1 or the ‘Swine flu’ virus in 2009. It is the only example in recent history where we managed to make a new vaccine in six months (because the winning candidate was very quickly identified, and Phase I, II and III were not necessary), and even then, the vaccine came too late to affect the second wave of infections. To end on a note of optimism, though, the more I read about this virus, the more I also think we may find a vaccine on a rather quick timeline because there are enough vaccines that have worked for similar viruses.
In the meanwhile, we must hope for the development of an efficient drug, and until then, manage very well the existing spread, with varying degrees of lockdown, testing and tracing, and social distancing measures. One drug that could help us a lot, as it looks promising, is Remdesivir. It has worked for SARS and MERS, and similar drugs are being used against hepatitis and HIV. It stops the multiplication of the virus. So, there’s a good chance that this one, or a variant, will work against the coronavirus. If you can give this at the first point of infection, it will work very well. It could be that this drug will be on the market by the fall.
Until then, we better get ready for a summer like no other. We may not see each other again for another couple of months, and when we do, it will have to be more like the Easter egg hunt, than sitting together at a table, close to each other. But on the bright side, we’re learning to use Zoom, WhatsApp and HouseParty, so we can all come together anyway.
— Dad, Guido Vanham
Guido Vanham is Professor of Virology at the University of Antwerp, and former Head of Virology at the Institute of Tropical Medicine in Antwerp, Belgium. His son, Peter Vanham, is Head of the International Media Council at the World Economic Forum, and a member of its COVID Taskforce.
This article is part of the COVID Action Platform for Media, a coalition of over 20 media from around the world. The Platform aims to create meaningful and constructive content on the COVID pandemic, and syndicates it through its media partners.
first give information virus fellow if coughing and sneezing while manufacturing of milk, biscuits, children food , cooldrinks, like any food items how long it will live that information give people going to manufacturing foods first tell me how long it will stay with food items like milk busicuit chocolates breads vegetables chps kurkurs noodles my number is 9296906906 be pls give like that research. To people to save from contaminated food items until vaccine we have to live first let me say contaminated food how long it virus live because some food items we are not cooking directly we eating that Time in this crucial switchvation we must know first very emergency because we don’t know who are in sick but they are manufacturing like children foods that Time they sneezing and coughing in that foods it will be happening please please analysis how many day will stay in food items like cooldrinks juice biscuits chocolates
As it was mentioned, vaccine trial will takes place in phases, 1,2,3 etc. After first phase, where very diluted ,low dose of vaccine is given , which will take a certain period, to get confirmed that ,immunity is developed or ended up inefficacy or other complications, or as it is very low or diluted form it will take very longer period, which again depends on personalised immunity, whatever it is, by the end of first phase, and before entering to 2nd phase we can come to a conclusion that it is safe to that level. Whether it has created immunity or not is a next question, because the development of immunity may take very longer duration for the low concentrated dose of vaccine.
After first phase why can’t we start giving vaccine to ppl , provided, being ruled out no complications were noticed.
Probably it will take longer period to develop immunity, which we can not anticipate,
We also cannot anticipate, personalised immunity capabilities.
The development of immunity may take indefinite period. That indefinite period, definitely , a valuable period. Because, we are sure of no complications, we don’t know it is creating immunity or not, but is sure at phase 3, it is creating immunity means (at measurable amount, which is clinically significant and useful to deal the present pandemic crisis).
But phase one should be utilised, not only as a green signal to go into phase 2 but also as a safe phase, it again depends, individual previous subclinical viral exposure, which in turn the DNA got embedded with innumerable subclinical viral exposure.
We cannot specify the phase one duration, sameway the phase 2.
It is always better to make use of phase one. Clinically.
To produce it into public. By the time 3phases gets over, the substantial damage to the mankind will takes place
Phase one level vaccine it utilised, whether it gives good results or not ,it has been proved that no complications were there.may not be immunity development, (immunity development may take very long period)
After 2nd phase of research, once it is confirmed ,no complications were there, again producing it into the public.
After 3rd phase, again, if till then 2nd phase people not developed, immunity, giving the specific vaccine.
Though it is economical burden, infront of the economical loss that is happening, that is not significant
The longer the duration to develop immunity, the more the safety, the more the specificity. I believe.
I have expressed my views I am soory if I am ignorant of the basics.
Wonderfully explained. Great article.
Datz it, 1 virus against billions of people….no close comfort, remain social distancing…..in 18 months there might be no one left in this world…..
Dear Professor Guido Vanham. Thank you for a very informative article. You have made the subject easy to understand without compromising on the technical facts. So readable, I could stop only when I reached the end! I am going to follow the Amanat and Krammer link to learn some more.