





There are four types of endemic human coronaviruses in the world—229E, NL63, OC43, and HKU1—and people across countries commonly get infected with these. According to experts, SARS-CoV-2 virus is soon becoming the fifth endemic human coronavirus. Once the supply bottlenecks of COVID-19 vaccines are overcome, the SARS-CoV-2 virus is supposed to become yet another manageable risk. However, the last 18 months have been nightmarish, where a new killer virus ran wild amongst an immunologically naive population.
China and India together constitute almost 40 percent of the world population, and both had imposed strict lockdowns early on, despite crushing economic costs. However, China—which had the first outbreak—was able to contain the virus much more efficiently than most other countries including India, and minimise COVID-19 deaths in the interim period when vaccines were awaited. With roughly comparable populations, the trajectory that the pandemic took in both countries, based on publicly available data, has been vastly different.
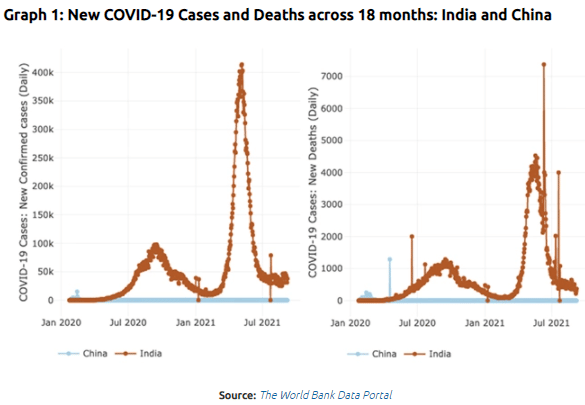
Quantifying COVID-19’s impact in China is a difficult task, due to the restrictions on information both related to the impact of the pandemic and countermeasures by the Chinese government. Given the authoritarian regime and the strict controls on information, any effort to compare the Chinese situation with other countries is fraught with challenges; however, despite having a vast and diverse population comparable to India, China was able to keep cases and deaths remarkably under check (Graph 1). At the same time, after having two devastating waves spread across over a year, many believe that India is going to see a surge in cases again.
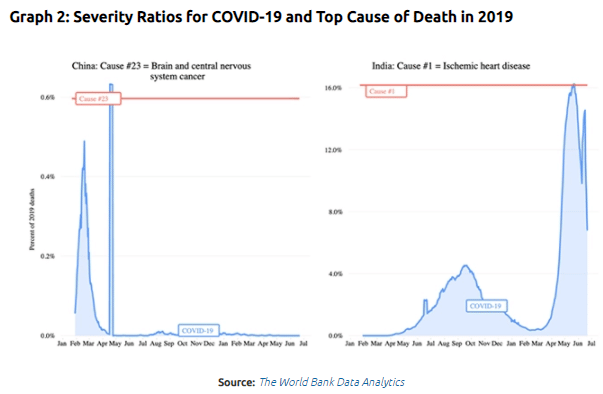
Comparative mortality burden from COVID-19 has shown a wide difference between India and China as well. Between January 2020 and September 2021, at the peak levels of daily reported COVID-19 deaths, COVID-19 mortality was comparable to the largest cause of death in India (Ischemic heart disease), and only the 23rd largest cause of death in China (Brain and central nervous system cancer), in a normal year. As represented in Graph 2, COVID-19 severity ratios express COVID-19 deaths in 2020-2021 in relation to deaths from all causes in 2019 as a 7-day average. According to the methodology, top-cause severity ratio(s) show cause-specific deaths in 2019 in relation to deaths from all causes in 2019 as a yearly average.
Centralised system of State
Ironically, it is the general lack of freedoms in China that contributed to its citizens having considerable freedom of movement when most parts of the world were reeling under lockdowns. Initially, China’s active suppression of facts about the origins of the pandemic, and its obfuscation of information about its spread had triggered world-wide criticism.
However, studies have shown that once the risks became clearer, the Chinese authorities locked down and reduced mobility at a scale unseen in the modern era. Apart from controlling population mobility, lack of test kits, masks, and personal protective equipment was another huge challenge for the government. A highly centralised political system made sure that China could reallocate resources, including human resources, quickly from regions that were less affected. A large number of medical volunteers were rushed into hotspots, which contributed to containment of the virus in a relatively short time. The lessons from the initial wave and containment were effectively used to suppress another outbreak in Beijing in June as well.
While being the source of almost infinite and highly centralised power, the Chinese Communist Party was also able to deploy its grassroots network as an effective arm of the government machinery itself, given the symbiotic relationship between the Party and Government structure. Analysts observe that the residential committees (RCs) played a crucial role in complementing the government machinery. These instruments of the Party were a key element ensuring effective governance and political control over the pandemic response on the ground.
China and India responded to the pandemic with an iron fist, using draconian public health measures. In China’s case, a population conditioned over the decades to meekly submit to an authoritarian state’s diktats helped tremendously. China had a population that has been conditioned to trust the government to do what it claimed. And the State responded with almost symbolic acts of power and resolve including building a mammoth hospital in two weeks, ordering its factories to scale up PPE manufacturing, ensuring compliance, and making COVID-19 treatment state-funded. Researchers suggest that controls over the movement and behaviour of people were implemented much more strictly in China because the population there is accustomed to living with authoritarianism, and they are seemingly more willing to make the trade-off between social order and social control. Research by the Institute of Chinese Studies found that the most striking aspect of China’s recovery was that the resumption of economic activity was achieved mainly by directives. The public health measures were implemented with precision within a command-and-control framework.
On the other hand, in India’s case, along with severe healthcare infrastructure constraints, the basic lack of trust—built over decades of underfunding within social sectors—in the State’s ability to provide support systems for the population affected the efficiency of implementation of its COVID-19 response. The contrast between the chaos in India and the authoritarian precision cannot be more stark than in the area of mobility control. Even as cases were mounting, authorities at the Centre, State and local levels in India were unwilling to or were unable to control political or religious gatherings of mass scale.
This resonates with recent research comparing public health containment measures in India and China, which found that the strict city-closure measures early on, aggressive screening, and tracking of detected cases helped control the population level spread while the country waited for vaccines. In contrast, enforcement of strict measures in India was patchy at best. In other words, population level compliance of public health measures was mandatory in China, while compliance was voluntary in India, and for that reason, the success of such measures hinged on individual risk perceptions of the leadership as well as the people.
In India, political reasons caused ineffective implementation; while in China even the pandemic response was politicised and used to suppress genuine dissent, as the case of Hong Kong demonstrated. Hong Kong used smart surveillance, quarantine and social-distancing measures, such as the use of face masks and school closures, to effectively cut coronavirus transmission. However, even in a situation of low transmission, China was accused of using the excuse of COVID-19 control measures to silence people’s protests.
There are studies that point out that China’s authoritarian political system and stricter information control, effectively restricted the circulation of fake news/rumours during the COVID-19 outbreak, when compared to other countries. The Chinese emphasised on ‘social responsibility’, ‘public security’ and ‘social order’ as justifications for censorships and government action. The parallels between the successful containment of the infodemic by the Chinese authorities and their breaking the chain of transmission of the actual SARS-CoV-2 virus are striking. In India, the effectiveness of countermeasures to the virus as well as infodemic was largely dependent on voluntary compliance by the population rather than enforcement by a muscular State.
Vaccine production
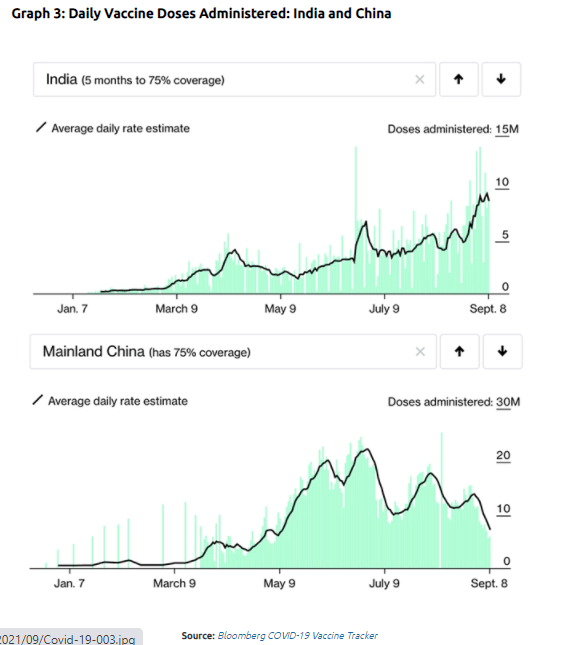
Scaling up of vaccine supplies was to be a key determinant of how fast a country could get back to normal. Even though it was the biggest vaccine manufacturer in the world pre-pandemic, India failed to scale up in time, whereas China increased vaccine production multifold over months, reflected in the mammoth vaccine coverage it has achieved within the country as well as abroad with its aggressive vaccine diplomacy efforts. As of 7th September, India constituting 17.7 percent of the world population has conducted 12.7 percent of the world’s COVID-19 vaccinations, while China with 18.2 percent of the world population has conducted a vastly higher 37.7 percent of vaccinations. India has had a slow start with vaccination and has neared a daily vaccination rate of 10 million only in September, while China had reached 10 million a day levels many months back (Graph 3). With India managing to overcome manufacturing bottlenecks, its path towards vaccinating all adults this year must have become easier. Interestingly, despite the infodemic around vaccines, an interview-based survey of young adults across 15 countries between August 31-September 6 showed that India along with China are the highest ranked in terms of vaccine confidence in the world.
Comparative research found that during the wait for vaccines, a containment strategy worked better than a mitigation strategy. Implementation of the initial containment strategy in India had only limited success in limiting the spread of the virus, which implied that the de-facto focus was on mitigation, which depended on an inadequately equipped public healthcare system. Thankfully, India being a young country, with about half the population under 25 years of age, certainly helped in keeping the overall human cost lower than what it could have been.
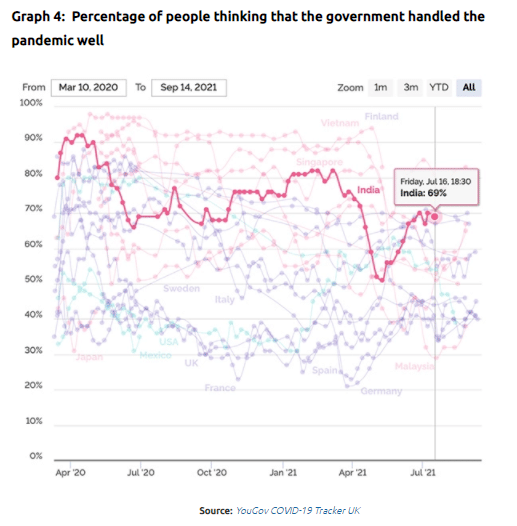
All factors considered, the stark contrast in terms of outcomes such as case and death burden between India and China in their respective approaches of pandemic response was a result of COVID-19 in India putting a part of the governance structure which was historically the weakest—its underfunded public healthcare system—through an extreme stress test. In China, the same authoritarian system which suppressed information about the pandemic initially, threw the full weight of the State apparatus behind containing the virus, and succeeded, till vaccine supplies were scaled up. It is undeniable that COVID-19’s human cost has been huge in India. However, somewhat counterintuitively, the percentage of citizens thinking that the government is handling the pandemic “very” or “somewhat” well has been consistently high in India, barring dips during the devastating waves, only to go up again (Graph 4). Understandably, the graph has no data from China.
Oommen C. Kurian @oommen is a Senior Fellow & Head of Health Initiative at ORF working on public health. Views are personal.
The article originally appeared on the Observer Research Foundation website. It has been republished with permission.